Das könnte Ihnen auch gefallen
- Atlanta Pssig Presentation To Pher Cbhs and PCDokument30 SeitenAtlanta Pssig Presentation To Pher Cbhs and PCRAHMAHNoch keine Bewertungen
- Isu, Kebijakan, Tantangan Patient Safety Serta Keselamatan Dan Kesehatan Kerja (K3) Dalam Pelayanan KesehatanDokument24 SeitenIsu, Kebijakan, Tantangan Patient Safety Serta Keselamatan Dan Kesehatan Kerja (K3) Dalam Pelayanan KesehatanCarl JungNoch keine Bewertungen
- Atlanta Pssig Presentation To Pher Cbhs and PCDokument30 SeitenAtlanta Pssig Presentation To Pher Cbhs and PCRAHMAHNoch keine Bewertungen
- Weaving Safety CultureDokument13 SeitenWeaving Safety CultureRAHMAHNoch keine Bewertungen
- Weaving Safety CultureDokument13 SeitenWeaving Safety CultureRAHMAHNoch keine Bewertungen
- KMK No. 432 TTG Pedoman Manajemen Kesehatan Dan Keselamatan Kerja (K3) Di Rumah SakitDokument15 SeitenKMK No. 432 TTG Pedoman Manajemen Kesehatan Dan Keselamatan Kerja (K3) Di Rumah SakitRigen Adi KowaraNoch keine Bewertungen
- Weaving Safety CultureDokument13 SeitenWeaving Safety CultureRAHMAHNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Organisation Study Report On Star PVC PipesDokument16 SeitenOrganisation Study Report On Star PVC PipesViswa Keerthi100% (1)
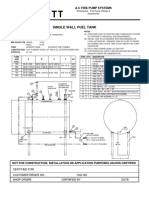
- Single Wall Fuel Tank: FP 2.7 A-C Fire Pump SystemsDokument1 SeiteSingle Wall Fuel Tank: FP 2.7 A-C Fire Pump Systemsricardo cardosoNoch keine Bewertungen
- "60 Tips On Object Oriented Programming" BrochureDokument1 Seite"60 Tips On Object Oriented Programming" BrochuresgganeshNoch keine Bewertungen
- Code Description DSMCDokument35 SeitenCode Description DSMCAnkit BansalNoch keine Bewertungen
- Proposal Semister ProjectDokument7 SeitenProposal Semister ProjectMuket AgmasNoch keine Bewertungen
- Indian Institute of Management KozhikodeDokument5 SeitenIndian Institute of Management KozhikodepranaliNoch keine Bewertungen
- Bank Statement AnalysisDokument26 SeitenBank Statement AnalysisAishwarya ManoharNoch keine Bewertungen
- Chapter 1 Qus OnlyDokument28 SeitenChapter 1 Qus OnlySaksharNoch keine Bewertungen
- Guidelines On Accreditation of CSOs (LSB Representation) - DILG MC 2019-72Dokument18 SeitenGuidelines On Accreditation of CSOs (LSB Representation) - DILG MC 2019-72Cedric Dequito100% (1)
- CORE Education Bags Rs. 120 Cr. Order From Gujarat Govt.Dokument2 SeitenCORE Education Bags Rs. 120 Cr. Order From Gujarat Govt.Sanjeev MansotraNoch keine Bewertungen
- Jurisdiction On Criminal Cases and PrinciplesDokument6 SeitenJurisdiction On Criminal Cases and PrinciplesJeffrey Garcia IlaganNoch keine Bewertungen
- Basic Electrical Design of A PLC Panel (Wiring Diagrams) - EEPDokument6 SeitenBasic Electrical Design of A PLC Panel (Wiring Diagrams) - EEPRobert GalarzaNoch keine Bewertungen
- 7th Kannada Science 01Dokument160 Seiten7th Kannada Science 01Edit O Pics StatusNoch keine Bewertungen
- Haryana Retial GarmentsDokument8 SeitenHaryana Retial Garmentssudesh.samastNoch keine Bewertungen
- Marketing ManagementDokument14 SeitenMarketing ManagementShaurya RathourNoch keine Bewertungen
- Legal Techniques (2nd Set)Dokument152 SeitenLegal Techniques (2nd Set)Karl Marxcuz ReyesNoch keine Bewertungen
- Fabric Bursting StrengthDokument14 SeitenFabric Bursting StrengthQaiseriqball100% (5)
- Project The Ant Ranch Ponzi Scheme JDDokument7 SeitenProject The Ant Ranch Ponzi Scheme JDmorraz360Noch keine Bewertungen
- MiniQAR MK IIDokument4 SeitenMiniQAR MK IIChristina Gray0% (1)
- Trinath Chigurupati, A095 576 649 (BIA Oct. 26, 2011)Dokument13 SeitenTrinath Chigurupati, A095 576 649 (BIA Oct. 26, 2011)Immigrant & Refugee Appellate Center, LLCNoch keine Bewertungen
- (Free Scores - Com) - Stumpf Werner Drive Blues en Mi Pour La Guitare 40562 PDFDokument2 Seiten(Free Scores - Com) - Stumpf Werner Drive Blues en Mi Pour La Guitare 40562 PDFAntonio FresiNoch keine Bewertungen
- LPM 52 Compar Ref GuideDokument54 SeitenLPM 52 Compar Ref GuideJimmy GilcesNoch keine Bewertungen
- Growatt SPF3000TL-HVM (2020)Dokument2 SeitenGrowatt SPF3000TL-HVM (2020)RUNARUNNoch keine Bewertungen
- Bob Wright's Declaration of BeingDokument1 SeiteBob Wright's Declaration of BeingBZ Riger100% (2)
- 1st Exam Practice Scratch (Answer)Dokument2 Seiten1st Exam Practice Scratch (Answer)Tang Hing Yiu, SamuelNoch keine Bewertungen
- Geneva IntrotoBankDebt172Dokument66 SeitenGeneva IntrotoBankDebt172satishlad1288Noch keine Bewertungen
- ATOMIC GAMING Technical Tutorial 1 - Drawing Game Statistics From Diversity Multigame StatisticsDokument4 SeitenATOMIC GAMING Technical Tutorial 1 - Drawing Game Statistics From Diversity Multigame StatisticsmiltoncgNoch keine Bewertungen
- Okuma Osp5000Dokument2 SeitenOkuma Osp5000Zoran VujadinovicNoch keine Bewertungen
- Asian Construction Dispute Denied ReviewDokument2 SeitenAsian Construction Dispute Denied ReviewJay jogs100% (2)
- Open Compute Project AMD Motherboard Roadrunner 2.1 PDFDokument36 SeitenOpen Compute Project AMD Motherboard Roadrunner 2.1 PDFakok22Noch keine Bewertungen