Das könnte Ihnen auch gefallen
- CPD, Dystocia, Fetal Distress OutputDokument8 SeitenCPD, Dystocia, Fetal Distress OutputJohn Dave AbranNoch keine Bewertungen
- CS Case PresentationDokument16 SeitenCS Case PresentationjisooNoch keine Bewertungen
- Ectopic PregnancyDokument65 SeitenEctopic PregnancyWen SilverNoch keine Bewertungen
- NCM 109 Prelims ReviewerDokument2 SeitenNCM 109 Prelims ReviewerReyna Chame GarcinezNoch keine Bewertungen
- Discharge PlanningDokument2 SeitenDischarge PlanningAthena Irish LastimosaNoch keine Bewertungen
- NCM107 - Chapter 04-Lesson 3 Postpartal CareDokument22 SeitenNCM107 - Chapter 04-Lesson 3 Postpartal CareJosephine LoriaNoch keine Bewertungen
- Meconium Aspiration Syndrome: DR Bob KlajoDokument17 SeitenMeconium Aspiration Syndrome: DR Bob KlajoBob John100% (1)
- NSDDokument44 SeitenNSDabyssodeep100% (1)
- Problems With Passenger and PowerDokument6 SeitenProblems With Passenger and PowerhoohooNoch keine Bewertungen
- HyperbilirubinemiaDokument49 SeitenHyperbilirubinemiaKeith LajotNoch keine Bewertungen
- Incompetent CervixDokument29 SeitenIncompetent CervixCyrelle Jen TorresNoch keine Bewertungen
- MCN Exam 2 Study Guide - CompleteDokument87 SeitenMCN Exam 2 Study Guide - CompleteColin MacKenzie100% (1)
- Complications With The Passenger 2Dokument77 SeitenComplications With The Passenger 2JudyNoch keine Bewertungen
- Assessment of Fetal Growth and DevelopmentDokument12 SeitenAssessment of Fetal Growth and Developmentaracelisurat100% (1)
- Prelim Examination MaternalDokument23 SeitenPrelim Examination MaternalAaron ConstantinoNoch keine Bewertungen
- Ectopic Pregnancy - PathophysiologyDokument1 SeiteEctopic Pregnancy - PathophysiologyMarimiel PagulayanNoch keine Bewertungen
- Chapter 11: Nursing Care Related To Assessment of Pregnant FamilyDokument7 SeitenChapter 11: Nursing Care Related To Assessment of Pregnant FamilyAlyssaGrandeMontimorNoch keine Bewertungen
- BubbleHe AssessmentDokument1 SeiteBubbleHe AssessmentVictoriaStoneHarrisNoch keine Bewertungen
- Cephalopelvic DisproportionDokument2 SeitenCephalopelvic DisproportionWirahadi SanjayaNoch keine Bewertungen
- Esarean Ction: Cadalin, Fremelen Rose Cedamon, CarloDokument18 SeitenEsarean Ction: Cadalin, Fremelen Rose Cedamon, CarloMonette Abalos MendovaNoch keine Bewertungen
- Bubble He Assessment: Vital SignsDokument11 SeitenBubble He Assessment: Vital SignsFregen Mae ApoyaNoch keine Bewertungen
- NCM 109 Care of Mother and Child at RiskDokument10 SeitenNCM 109 Care of Mother and Child at RiskMia Fe Cuaya Lorenzo100% (1)
- Stages of LaborDokument14 SeitenStages of LaborKimberly CostalesNoch keine Bewertungen
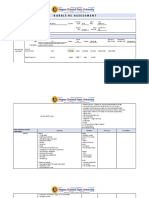
- Health Teaching Plan For Newborn ScreeningDokument4 SeitenHealth Teaching Plan For Newborn ScreeningPrincess Pauline AbrasaldoNoch keine Bewertungen
- Prob With The PowerDokument4 SeitenProb With The PowerPauline Navarro100% (1)
- NCM 109 2023 F-ACAD-29 - Syllabus Template (Rev 6)Dokument63 SeitenNCM 109 2023 F-ACAD-29 - Syllabus Template (Rev 6)Joyce EricaNoch keine Bewertungen
- Case PresDokument100 SeitenCase PresJoj BagnateNoch keine Bewertungen
- InstrumentsDokument7 SeitenInstrumentsOllet Athive NatacabNoch keine Bewertungen
- Intrapartal PeriodDokument2 SeitenIntrapartal PeriodLeah ElizabethNoch keine Bewertungen
- Clinical Face Sheet: G3P2, Pregnancy Uterine (PU), 37 Weeks and 5 Days AOG, Previous CS IIDokument14 SeitenClinical Face Sheet: G3P2, Pregnancy Uterine (PU), 37 Weeks and 5 Days AOG, Previous CS IICezanne CruzNoch keine Bewertungen
- RLE 109 Group 4 Case Analysis in MastitisDokument20 SeitenRLE 109 Group 4 Case Analysis in MastitisEugene MananganNoch keine Bewertungen
- Incompetent CervixDokument5 SeitenIncompetent CervixNaidin Catherine De Guzman-Alcala100% (1)
- Case Presentation 12319Dokument52 SeitenCase Presentation 12319Salazar DaisyNoch keine Bewertungen
- Hyperemesis GravidarumDokument36 SeitenHyperemesis GravidarumjanissNoch keine Bewertungen
- Fluid and Electrolytes Session 1-8Dokument17 SeitenFluid and Electrolytes Session 1-8Angie100% (1)
- Labor & DeliveryDokument14 SeitenLabor & DeliveryNiña Eleana FranciscoNoch keine Bewertungen
- Uterine Atony: Group 3Dokument23 SeitenUterine Atony: Group 3Trisha Mae MarquezNoch keine Bewertungen
- Case Study Missed Miscarriage Dilation and CurettageDokument48 SeitenCase Study Missed Miscarriage Dilation and CurettageEsther Ellise AbundoNoch keine Bewertungen
- Nursing Care of Family During Labor and BirthDokument18 SeitenNursing Care of Family During Labor and BirthAudreySalvadorNoch keine Bewertungen
- Advance Practice in Maternal and Child Nursing 1 High Risk Pregnancy: Nursing Care of A Family Experiencing A Pregnancy Complication From A Pre-Existing or Newly Acquired IllnessDokument31 SeitenAdvance Practice in Maternal and Child Nursing 1 High Risk Pregnancy: Nursing Care of A Family Experiencing A Pregnancy Complication From A Pre-Existing or Newly Acquired Illnessallanrnmanaloto100% (2)
- Nursing Care of The Family Experiencing A Sudden Pregnancy ComplicationDokument7 SeitenNursing Care of The Family Experiencing A Sudden Pregnancy ComplicationDacillo GailleNoch keine Bewertungen
- HANDOUTDokument7 SeitenHANDOUTRainier IbarretaNoch keine Bewertungen
- A. Dystocia: Problems With PowerDokument48 SeitenA. Dystocia: Problems With PowerPauline GarciaNoch keine Bewertungen
- CAJA, RENZO GABRIEL, BSN 2-1 NCM109-Midterm ModuleDokument14 SeitenCAJA, RENZO GABRIEL, BSN 2-1 NCM109-Midterm ModuleRenzo GabrielNoch keine Bewertungen
- Case Study 7Dokument29 SeitenCase Study 7Hanniel MontecalboNoch keine Bewertungen
- Case 5Dokument18 SeitenCase 5Brian Arthur LeysonNoch keine Bewertungen
- Intrapartum QuestionsDokument24 SeitenIntrapartum QuestionsAnonymous ZduHBgNoch keine Bewertungen
- COURSE in The WARD Interhospital FinalDokument8 SeitenCOURSE in The WARD Interhospital Finalkimadlo656Noch keine Bewertungen
- wk8 Nursing Care of A Family When A Child Has An Immune Disorders Part 2Dokument32 Seitenwk8 Nursing Care of A Family When A Child Has An Immune Disorders Part 2claire yowsNoch keine Bewertungen
- Prenatal AssessmentDokument29 SeitenPrenatal AssessmentPaula Janine Barroga100% (1)
- Pathophysiology-Threatened MiscarriageDokument1 SeitePathophysiology-Threatened MiscarriageMoses Gabriel ValledorNoch keine Bewertungen
- EclampsiaDokument47 SeitenEclampsiarranindyaprabasaryNoch keine Bewertungen
- Intrapartum NCM 107Dokument8 SeitenIntrapartum NCM 107Kimberly Sharah Mae FortunoNoch keine Bewertungen
- NCM 109 Resource UnitDokument51 SeitenNCM 109 Resource UnitDaryl Adrian RecaidoNoch keine Bewertungen
- A Contracture in Any of These Can Result in CPDDokument7 SeitenA Contracture in Any of These Can Result in CPDMika SamsonNoch keine Bewertungen
- Hemorrhagic Complications During Labor and Management - MoralDokument45 SeitenHemorrhagic Complications During Labor and Management - MoralAngel Mae BaborNoch keine Bewertungen
- Complications During Labor and Delivery - HardDokument19 SeitenComplications During Labor and Delivery - Hardkrizele ann santosNoch keine Bewertungen
- Nursing Care Management 102Dokument14 SeitenNursing Care Management 102Annabelle LuceroNoch keine Bewertungen
- Antepartum HaemorrhageDokument33 SeitenAntepartum HaemorrhageMedy WedhanggaNoch keine Bewertungen
- Savage Cyberpunk 2020Dokument14 SeitenSavage Cyberpunk 2020dmage_uNoch keine Bewertungen
- Dela Cruz vs. Atty. DimaanoDokument8 SeitenDela Cruz vs. Atty. DimaanoMarga CastilloNoch keine Bewertungen
- Permanently End Premature EjaculationDokument198 SeitenPermanently End Premature EjaculationZachary Leow100% (5)
- Brochure Selector Guide EN-web-protectedDokument16 SeitenBrochure Selector Guide EN-web-protectedPierre-Olivier MouthuyNoch keine Bewertungen
- Apollo Hospital Chennai: NO: 16, BSNL TELESHOPPE, Greams Road 044 2999 1606Dokument9 SeitenApollo Hospital Chennai: NO: 16, BSNL TELESHOPPE, Greams Road 044 2999 1606Manas ChandaNoch keine Bewertungen
- A Proposed Approach To Handling Unbounded Dependencies in Automatic ParsersDokument149 SeitenA Proposed Approach To Handling Unbounded Dependencies in Automatic ParsersRamy Al-GamalNoch keine Bewertungen
- Dlis103 Library Classification and Cataloguing TheoryDokument110 SeitenDlis103 Library Classification and Cataloguing Theoryabbasimuhammadwaqar74Noch keine Bewertungen
- Intj MbtiDokument17 SeitenIntj Mbti1985 productionNoch keine Bewertungen
- Or SuperDokument2 SeitenOr SuperJac BacNoch keine Bewertungen
- Account StatementDokument12 SeitenAccount StatementbadramostuNoch keine Bewertungen
- Republic of The Philippines: Paulene V. Silvestre Personal DevelopmentDokument3 SeitenRepublic of The Philippines: Paulene V. Silvestre Personal DevelopmentPau SilvestreNoch keine Bewertungen
- Notice: Agency Information Collection Activities Proposals, Submissions, and ApprovalsDokument2 SeitenNotice: Agency Information Collection Activities Proposals, Submissions, and ApprovalsJustia.comNoch keine Bewertungen
- The Watchmen Novel AnalysisDokument10 SeitenThe Watchmen Novel AnalysisFreddy GachecheNoch keine Bewertungen
- 555LDokument8 Seiten555LVictor Mamani VargasNoch keine Bewertungen
- CABE Space - A Guide To Producing Park and Green Space Management PlansDokument48 SeitenCABE Space - A Guide To Producing Park and Green Space Management PlansbenconnolleyNoch keine Bewertungen
- ERF 2019 0128 H160 Noise CertificationDokument10 SeitenERF 2019 0128 H160 Noise CertificationHelimanualNoch keine Bewertungen
- 2019 National Innovation PoliciesDokument98 Seiten2019 National Innovation PoliciesRashmi SinghNoch keine Bewertungen
- Tle9cookery q1 m7 Presentingandstoringarangeofappetizer v2Dokument30 SeitenTle9cookery q1 m7 Presentingandstoringarangeofappetizer v2Almaira SumpinganNoch keine Bewertungen
- Brochure For New HiresDokument11 SeitenBrochure For New HiresroseNoch keine Bewertungen
- Lesson 20 PerdevDokument7 SeitenLesson 20 PerdevIvan Joshua RemosNoch keine Bewertungen
- Gonzales Cannon Feb 28 IssueDokument40 SeitenGonzales Cannon Feb 28 IssueGonzales CannonNoch keine Bewertungen
- Lipoproteins in Diabetes Mellitus: Alicia J. Jenkins Peter P. Toth Timothy J. Lyons EditorsDokument468 SeitenLipoproteins in Diabetes Mellitus: Alicia J. Jenkins Peter P. Toth Timothy J. Lyons EditorsFELELNoch keine Bewertungen
- Collec The PassportDokument2 SeitenCollec The PassportvijikaNoch keine Bewertungen
- Listening Test Sweeney Todd, Chapter 4: 1 C. Zwyssig-KliemDokument3 SeitenListening Test Sweeney Todd, Chapter 4: 1 C. Zwyssig-KliemCarole Zwyssig-KliemNoch keine Bewertungen
- MNDCS-2024 New3 - 231101 - 003728Dokument3 SeitenMNDCS-2024 New3 - 231101 - 003728Dr. Farida Ashraf AliNoch keine Bewertungen
- The Fat Cat Called PatDokument12 SeitenThe Fat Cat Called PatAlex ArroNoch keine Bewertungen
- IHE ITI Suppl XDS Metadata UpdateDokument76 SeitenIHE ITI Suppl XDS Metadata UpdateamNoch keine Bewertungen
- International Banking & Foreign Exchange ManagementDokument4 SeitenInternational Banking & Foreign Exchange ManagementAnupriya HiranwalNoch keine Bewertungen
- Kuis 4Dokument10 SeitenKuis 4Deri AntoNoch keine Bewertungen
- 2.peace Treaties With Defeated PowersDokument13 Seiten2.peace Treaties With Defeated PowersTENDAI MAVHIZANoch keine Bewertungen