Das könnte Ihnen auch gefallen
- 12 DHF DRDokument56 Seiten12 DHF DRdokteraanNoch keine Bewertungen
- DengueDokument36 SeitenDengueMohd Alfian Awang Ku LekNoch keine Bewertungen
- Dengue PPT Update 2Dokument73 SeitenDengue PPT Update 2Hakuna MatataNoch keine Bewertungen
- Dengue FeverDokument44 SeitenDengue FeverTrebor Santos100% (2)
- (29 August, 2016) Department of General Medicine PIMS IslamabadDokument43 Seiten(29 August, 2016) Department of General Medicine PIMS IslamabadwaseemNoch keine Bewertungen
- Joel Vasanth PeterDokument38 SeitenJoel Vasanth PeterJoelPeterNoch keine Bewertungen
- CSS DHFDokument40 SeitenCSS DHFDina SofianaNoch keine Bewertungen
- Locally Endemic DiseasesDokument23 SeitenLocally Endemic DiseasesERMIAS, ZENDY I.Noch keine Bewertungen
- Dengue Fever by DR - RadheDokument39 SeitenDengue Fever by DR - RadheRAMJIBAN YADAVNoch keine Bewertungen
- Dengue: (Mosquito Borne)Dokument45 SeitenDengue: (Mosquito Borne)Sibi PalanisamyNoch keine Bewertungen
- Dengue Prevention and Control Program - Department of Health WebsiteDokument4 SeitenDengue Prevention and Control Program - Department of Health WebsiteJL CalvinNoch keine Bewertungen
- Dengue Fever by Prof M Ali KhanDokument36 SeitenDengue Fever by Prof M Ali KhanVina MuspitaNoch keine Bewertungen
- DengueDokument9 SeitenDengueWinna Gonato100% (2)
- 94 JMSCRDokument3 Seiten94 JMSCRmaria lisaNoch keine Bewertungen
- Arboviral Diseases and Dengue FinalDokument73 SeitenArboviral Diseases and Dengue FinalBinayaNoch keine Bewertungen
- Management of Dengue and Dengue Haemorrhagic FeverDokument17 SeitenManagement of Dengue and Dengue Haemorrhagic FevernjiexxNoch keine Bewertungen
- 853 PDFDokument122 Seiten853 PDFTammy StephanieNoch keine Bewertungen
- Communicable Diseases: Roberto M. Salvador Jr. R.N.,M.D. Infectious and Tropical Disease SpecialistDokument846 SeitenCommunicable Diseases: Roberto M. Salvador Jr. R.N.,M.D. Infectious and Tropical Disease SpecialistGrn Mynjrkxz100% (1)
- Denguefinalpdf-170803082145 2Dokument74 SeitenDenguefinalpdf-170803082145 2L. HusnaNoch keine Bewertungen
- Dengue FeverDokument24 SeitenDengue FeverDrSlayer100% (1)
- Dengue 121008123903 Phpapp02Dokument34 SeitenDengue 121008123903 Phpapp02maharshi mNoch keine Bewertungen
- By Benelyne MDokument9 SeitenBy Benelyne MCharm TanyaNoch keine Bewertungen
- Doh Program PrintDokument7 SeitenDoh Program PrintStrawberry Mae DipasupilNoch keine Bewertungen
- Dengue MedscapeDokument36 SeitenDengue Medscapejeanne_mbNoch keine Bewertungen
- Dengue PPT YaarDokument21 SeitenDengue PPT YaarY ShouryaNoch keine Bewertungen
- DengueDokument7 SeitenDengueHafsah MangarunNoch keine Bewertungen
- Dengue Feve1Dokument10 SeitenDengue Feve1Santhosh KumarNoch keine Bewertungen
- Dengue Fever Case StudyDokument5 SeitenDengue Fever Case StudyJen Faye Orpilla100% (1)
- Dengue FeverDokument53 SeitenDengue FeverAnnsha VeiNoch keine Bewertungen
- Dengue Fever by Prof M Ali KhanDokument36 SeitenDengue Fever by Prof M Ali Khanmaha rNoch keine Bewertungen
- Decee Marie T. Miranda Saint Mary'S University BSN Group6: Dengue Hemorrhagic FeverDokument5 SeitenDecee Marie T. Miranda Saint Mary'S University BSN Group6: Dengue Hemorrhagic FeverJeff Mac Rae RamosNoch keine Bewertungen
- Dengue 2Dokument56 SeitenDengue 2Eliz Codilla-SyNoch keine Bewertungen
- Dengue Fever by Prof M Ali KhanDokument36 SeitenDengue Fever by Prof M Ali KhanAnonymous uGbcVSJTDgNoch keine Bewertungen
- Journal Reading: Ade Cahyo Islami Dewinta Putri UtamiDokument17 SeitenJournal Reading: Ade Cahyo Islami Dewinta Putri UtamiAde Cahyo IslamiNoch keine Bewertungen
- Dengue Insight DR Amit Johari Edited 2020Dokument82 SeitenDengue Insight DR Amit Johari Edited 2020Vedehi BansalNoch keine Bewertungen
- Mengenali Kegawatan Dengue 2013Dokument40 SeitenMengenali Kegawatan Dengue 2013Fatahillah NazarNoch keine Bewertungen
- BogderDokument31 SeitenBogderDimitri EroticoNoch keine Bewertungen
- Aetiology, Pathophysiology and Diagnosis of Dengue Infection: DR Lee Oi Wah Peg. Perubatan Ud54Dokument40 SeitenAetiology, Pathophysiology and Diagnosis of Dengue Infection: DR Lee Oi Wah Peg. Perubatan Ud54EzraManzanoNoch keine Bewertungen
- Dengue Fever in PregnancyDokument36 SeitenDengue Fever in PregnancyShoaib Akhtar100% (1)
- Dengue Fever4Dokument23 SeitenDengue Fever4Shanthi Jaggala Shanthi YadavNoch keine Bewertungen
- Refreshing DHFDokument13 SeitenRefreshing DHFNia Nurhayati ZakiahNoch keine Bewertungen
- DengueDokument43 SeitenDenguePed SilvestreNoch keine Bewertungen
- Dengue Case DiscussionDokument16 SeitenDengue Case DiscussionCorinne Fatima de AsisNoch keine Bewertungen
- DengueDokument34 SeitenDengueNa YamzonNoch keine Bewertungen
- Communicable DiseasesDokument7 SeitenCommunicable DiseasesRaisa Robelle Quicho100% (1)
- Presentation On DengueDokument39 SeitenPresentation On DenguearmanNoch keine Bewertungen
- Dengue UpdatesDokument6 SeitenDengue UpdatesGina Mea Charel DawatonNoch keine Bewertungen
- DENGUE Hemorrhagic FeverDokument4 SeitenDENGUE Hemorrhagic FeverTonee Marie GabrielNoch keine Bewertungen
- Gil P. Soriano, RN, MhpedDokument24 SeitenGil P. Soriano, RN, MhpedGil Platon SorianoNoch keine Bewertungen
- Dengue Prevention and Control ProgramDokument7 SeitenDengue Prevention and Control ProgramXandrienne Joy ArañoNoch keine Bewertungen
- Dengue Fever: Thrombocytopenic Purpura"Dokument8 SeitenDengue Fever: Thrombocytopenic Purpura"christian quiaoitNoch keine Bewertungen
- Case Presentation 1Dokument37 SeitenCase Presentation 1Safoora RafeeqNoch keine Bewertungen
- Fortfolio of ARIFDokument20 SeitenFortfolio of ARIFWaqas AhmadNoch keine Bewertungen
- Dengue 3Dokument9 SeitenDengue 3Bernadette Collamar Dela CruzNoch keine Bewertungen
- Clinical Management Protocol PDFDokument7 SeitenClinical Management Protocol PDFAJEET KUMAR PANDEYNoch keine Bewertungen
- Case Study: Rle: Dengue Hemorrhagic FeverDokument7 SeitenCase Study: Rle: Dengue Hemorrhagic FeverNikka Moreen Dagdag0% (1)
- DengueDokument65 SeitenDengueShajahan SideequeNoch keine Bewertungen
- Dengue Fever 4Dokument65 SeitenDengue Fever 4Roshandiep GillNoch keine Bewertungen
- DengueDokument35 SeitenDengueJessy HanNoch keine Bewertungen
- Med Fact SheetDokument2 SeitenMed Fact SheetushapadminivadivelswamyNoch keine Bewertungen
- PDFDokument4 SeitenPDFushapadminivadivelswamyNoch keine Bewertungen
- Śrī Jagannāthā Akam: (Uttered by Śrī Caitanya Mahāprabhu)Dokument5 SeitenŚrī Jagannāthā Akam: (Uttered by Śrī Caitanya Mahāprabhu)ushapadminivadivelswamyNoch keine Bewertungen
- ALSANGEDY BULLETS FOR PACES HypogammaglobulinemiaDokument2 SeitenALSANGEDY BULLETS FOR PACES HypogammaglobulinemiaushapadminivadivelswamyNoch keine Bewertungen
- Sri Dakshinamurthy Sahasranamam Stotram and Namavali - Compressed PDFDokument32 SeitenSri Dakshinamurthy Sahasranamam Stotram and Namavali - Compressed PDFushapadminivadivelswamyNoch keine Bewertungen
- Sri Dakshinamurthy Sahasranamam Stotram and Namavali - Compressed PDFDokument32 SeitenSri Dakshinamurthy Sahasranamam Stotram and Namavali - Compressed PDFushapadminivadivelswamyNoch keine Bewertungen
- All Things Come by The Grace of God-Ralph Waldo EmersonDokument43 SeitenAll Things Come by The Grace of God-Ralph Waldo EmersonushapadminivadivelswamyNoch keine Bewertungen
- GIRL Child DayDokument12 SeitenGIRL Child DayushapadminivadivelswamyNoch keine Bewertungen
- Attitude Towards PatientsDokument28 SeitenAttitude Towards PatientsushapadminivadivelswamyNoch keine Bewertungen
- 5 Major Swimming Strokes: Grade 12 PE and HealthDokument11 Seiten5 Major Swimming Strokes: Grade 12 PE and HealthJack Daniel CandelarioNoch keine Bewertungen
- Stanley 25 Amp Automatic Battery Charger BC25BS ManualDokument12 SeitenStanley 25 Amp Automatic Battery Charger BC25BS ManualJoe ZhaoNoch keine Bewertungen
- SST LifeDokument3 SeitenSST Liferaj_kr1078Noch keine Bewertungen
- Armour Pro ManualDokument7 SeitenArmour Pro ManualadiNoch keine Bewertungen
- Savio v. Peterson ComplaintDokument15 SeitenSavio v. Peterson ComplaintChicago TribuneNoch keine Bewertungen
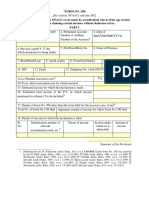
- New Form 12BBDokument2 SeitenNew Form 12BBramanNoch keine Bewertungen
- B I F Mukhopadhyay2019Dokument84 SeitenB I F Mukhopadhyay2019deshmukhgeolNoch keine Bewertungen
- Natural Gas EngineeringDokument51 SeitenNatural Gas EngineeringMusa favourNoch keine Bewertungen
- Ôn luyện cấp tốc chứng chỉ Tiếng Anh B1 B2 LH:0907.286.606Dokument10 SeitenÔn luyện cấp tốc chứng chỉ Tiếng Anh B1 B2 LH:0907.286.606Sĩ Phong100% (1)
- Caring Theories: Jaime R. Soriano - RN.RM - MSN.RTDokument56 SeitenCaring Theories: Jaime R. Soriano - RN.RM - MSN.RTMarcelle HolderNoch keine Bewertungen
- Bag Bath Return Demo For NursingDokument4 SeitenBag Bath Return Demo For Nursingjerica abesamisNoch keine Bewertungen
- 293005Dokument10 Seiten293005elsayedNoch keine Bewertungen
- SSC CHSL Classification PDF Part 2 Eng 64Dokument11 SeitenSSC CHSL Classification PDF Part 2 Eng 64SarveshNoch keine Bewertungen
- Gazpromneft Reductor CLP - 68, 100, 150, 220, 320, 460 and 680Dokument2 SeitenGazpromneft Reductor CLP - 68, 100, 150, 220, 320, 460 and 680Jonathan HansenNoch keine Bewertungen
- Madness Rules For RPGDokument20 SeitenMadness Rules For RPGKaiser Julianus Apostata100% (1)
- AssamerrrDokument15 SeitenAssamerrrVipul SharmaNoch keine Bewertungen
- Panduan Pelaksanaan Pemeriksaan Radiografi Kedokteran Gigi Pada Pasien AnakDokument5 SeitenPanduan Pelaksanaan Pemeriksaan Radiografi Kedokteran Gigi Pada Pasien AnakFebriani SerojaNoch keine Bewertungen
- V Unit - Wireless Network SecurityDokument22 SeitenV Unit - Wireless Network SecurityBRINDHA C it2018Noch keine Bewertungen
- Total Physical ResponseDokument7 SeitenTotal Physical ResponseDesak RossyanaNoch keine Bewertungen
- Nebosh Igc1 PDFDokument3 SeitenNebosh Igc1 PDFNoman HassanNoch keine Bewertungen
- Module 2 in Forensic BallisticsDokument9 SeitenModule 2 in Forensic Ballisticscriminologyalliance100% (2)
- AHA - Working On Slope RoofDokument2 SeitenAHA - Working On Slope RoofTopsun EnergyNoch keine Bewertungen
- Pranayam inDokument19 SeitenPranayam inSreeraj Guruvayoor SNoch keine Bewertungen
- 1 ReproductioninOrganismsDokument22 Seiten1 ReproductioninOrganismsPriNce KhatriNoch keine Bewertungen
- ELI 250c: Mortara'S Next Generation 12-Lead ElectrocardiographsDokument2 SeitenELI 250c: Mortara'S Next Generation 12-Lead ElectrocardiographszainalfikraNoch keine Bewertungen
- A Brief Note On Plants of Medicinal Importance To LivestockDokument84 SeitenA Brief Note On Plants of Medicinal Importance To LivestockSunil100% (1)
- 05.08 Saidkhasan SadievDokument2 Seiten05.08 Saidkhasan SadievjaborNoch keine Bewertungen
- Pharmaceutical Analysis (Proposed) Syllabus - Effective From The Session 2017-18Dokument22 SeitenPharmaceutical Analysis (Proposed) Syllabus - Effective From The Session 2017-18neeraj dasNoch keine Bewertungen
- 1 Yemen's Humanitarian Nightmare The Real Roots of The Conflict by Asher OrkabyDokument10 Seiten1 Yemen's Humanitarian Nightmare The Real Roots of The Conflict by Asher OrkabyLilia Archbold100% (1)
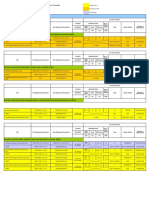
- T301 Summary of Pump Control PanelsDokument10 SeitenT301 Summary of Pump Control PanelsRanjani SNoch keine Bewertungen