Das könnte Ihnen auch gefallen
- Introduction To MidwiferyDokument42 SeitenIntroduction To MidwiferyAnnapurna Dangeti100% (5)
- Unit 1 - Introduction To MidwiferyDokument25 SeitenUnit 1 - Introduction To Midwiferypriya100% (1)
- Unit I - Introduction-to-Midwifery-Obstetrical-NursingDokument43 SeitenUnit I - Introduction-to-Midwifery-Obstetrical-NursingN. Siva100% (8)
- Ethics in Midwifery PracticeDokument42 SeitenEthics in Midwifery PracticeDivya Grace95% (19)
- Midwifery SkillsDokument416 SeitenMidwifery SkillsandrenwarholNoch keine Bewertungen
- Management of The First Stage of Labour LectureDokument48 SeitenManagement of The First Stage of Labour LectureJSeashark100% (3)
- High RiskDokument38 SeitenHigh RiskDiana Rose R. Ulep100% (2)
- Female PelvisDokument41 SeitenFemale Pelvissanthiyasandy100% (6)
- Common Legal Issue in Midwifery PracticeDokument14 SeitenCommon Legal Issue in Midwifery Practicelieynna4996100% (3)
- Introduction To OBGDokument23 SeitenIntroduction To OBGsindhujojo100% (1)
- Obstetrics N Gynaec Nursing PDFDokument12 SeitenObstetrics N Gynaec Nursing PDFSijo Muthukad M100% (1)
- Basic Concepts in MidwiferyDokument4 SeitenBasic Concepts in MidwiferyNileena Krishna100% (2)
- MINOR DISORDERS OF PREGNANCY FinalDokument6 SeitenMINOR DISORDERS OF PREGNANCY FinalChedupLepcha100% (7)
- Unit-2 Antenatal AssessmentDokument16 SeitenUnit-2 Antenatal AssessmentAnil Patel100% (5)
- Managament of The 2nd Stage of LabourDokument53 SeitenManagament of The 2nd Stage of LabourJSeashark100% (1)
- 4th Year - Unit 5 - Pharmacotherapeutics in Obstetrics 1Dokument13 Seiten4th Year - Unit 5 - Pharmacotherapeutics in Obstetrics 1Rupa Ghosh100% (1)
- Mechanism of LabourDokument10 SeitenMechanism of LabourMithlesh Dewangan100% (4)
- Medical and Surgical Complication in PregnancyDokument29 SeitenMedical and Surgical Complication in PregnancyVictor-Gabriel Rugina0% (1)
- National College of Nursing: Procedure ONDokument6 SeitenNational College of Nursing: Procedure ONSumit Yadav100% (1)
- Placenta ChecklistDokument2 SeitenPlacenta ChecklistNidhi Shivam Ahlawat100% (3)
- Diagnosis of PregnancyDokument47 SeitenDiagnosis of Pregnancypriyanka100% (2)
- Placenta DevelopmentDokument74 SeitenPlacenta DevelopmentEllagEsz33% (3)
- PGD MidwiferyDokument164 SeitenPGD MidwiferyVincent Quiña Piga100% (12)
- Government College of Nursing: Procedure ONDokument6 SeitenGovernment College of Nursing: Procedure ONpriyanka100% (5)
- A Comprehensive Textbook of Midwifery and Gynecological Nursing by Annamma Jacob 935025557x PDFDokument5 SeitenA Comprehensive Textbook of Midwifery and Gynecological Nursing by Annamma Jacob 935025557x PDFDev Ray70% (20)
- The Midwifery CurriculumDokument41 SeitenThe Midwifery Curriculummega surya100% (1)
- Preconception Care & Planned ParenthoodDokument7 SeitenPreconception Care & Planned ParenthoodDelphy Varghese86% (7)
- Genital Tract InjuriesDokument24 SeitenGenital Tract InjuriesManisha ThakurNoch keine Bewertungen
- 1 High Risk Pregnancy Assessment and ManagementDokument48 Seiten1 High Risk Pregnancy Assessment and ManagementNeelofur Ibran Ali80% (5)
- Antenatal Examination According To WHODokument6 SeitenAntenatal Examination According To WHOManisha ThakurNoch keine Bewertungen
- Learning Objectives of MidwiferyDokument2 SeitenLearning Objectives of Midwiferyangel panchal100% (1)
- Physiology of 1st Stage of LaborDokument134 SeitenPhysiology of 1st Stage of LaborVijith.V.kumar50% (2)
- Augmentation of LabourDokument45 SeitenAugmentation of LabourLamnunnem HaokipNoch keine Bewertungen
- Gynecological ProceduresDokument17 SeitenGynecological Proceduresjeelani saima100% (5)
- Perineal and Cervical TearsDokument43 SeitenPerineal and Cervical TearsN. SivaNoch keine Bewertungen
- MCQ On MenopauseDokument4 SeitenMCQ On Menopausesalamred100% (3)
- Female PelvisDokument18 SeitenFemale PelvisNeelofur Ibran Ali100% (1)
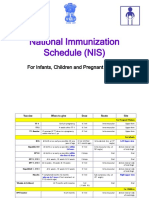
- National Immunization Schedule (NIS) : For Infants, Children and Pregnant WomenDokument13 SeitenNational Immunization Schedule (NIS) : For Infants, Children and Pregnant WomenPrabir Kumar Chatterjee100% (1)
- Seminar On Physiology of PuerperiumDokument15 SeitenSeminar On Physiology of Puerperiumvarshasharma05100% (3)
- Unit 3 Admission Procedure of Women in LabourDokument30 SeitenUnit 3 Admission Procedure of Women in LabourNishaThakuriNoch keine Bewertungen
- Female PelvisDokument4 SeitenFemale PelvisAnnapurna Dangeti100% (1)
- APHDokument107 SeitenAPHbaby100% (2)
- Lesson Plan Antenatal AssessmentDokument5 SeitenLesson Plan Antenatal AssessmentDelphy Varghese67% (3)
- Role and Scope of Midwifery PracticeDokument23 SeitenRole and Scope of Midwifery Practicesweta100% (1)
- Independent Midwifery PracticeDokument18 SeitenIndependent Midwifery Practiceneeta rajesh bhide100% (3)
- Malpositions and Malpresentations FinalDokument47 SeitenMalpositions and Malpresentations Finalsanthiyasandy82% (11)
- Introduction To Concept of Obstetrical NSGDokument11 SeitenIntroduction To Concept of Obstetrical NSGswethashaki100% (2)
- Obg Course PlanDokument4 SeitenObg Course PlanDelphy VargheseNoch keine Bewertungen
- Antepartum HemorrhageDokument21 SeitenAntepartum HemorrhageNidhi SharmaNoch keine Bewertungen
- Procedure On Vaginal ExaminationDokument7 SeitenProcedure On Vaginal ExaminationPriya100% (2)
- Cervical DystociaDokument22 SeitenCervical DystociaBaldau TiwariNoch keine Bewertungen
- The Average Blood Loss Following Vaginal Delivery, Cesarean Delivery and Cesarean Hysterectomy Is 500 ML, 1000 ML and 1500 ML RespectivelyDokument11 SeitenThe Average Blood Loss Following Vaginal Delivery, Cesarean Delivery and Cesarean Hysterectomy Is 500 ML, 1000 ML and 1500 ML RespectivelypriyankaNoch keine Bewertungen
- Contracted PelvisDokument13 SeitenContracted PelvisCuteness Romney100% (1)
- Essay Q's Obs and Gyn 2Dokument2 SeitenEssay Q's Obs and Gyn 2whoosh200886% (7)
- Injuries To The Birth CanalDokument67 SeitenInjuries To The Birth CanalnamitaNoch keine Bewertungen
- Contemprory Issues in ObstetricsDokument6 SeitenContemprory Issues in ObstetricsDelphy Varghese100% (1)
- Neuromuscular BlockersDokument25 SeitenNeuromuscular BlockersAbdelrahman GalalNoch keine Bewertungen
- Pharmaceutical and Clinical Study of Kumkumadi Cream Prepared Using Kwath As Water Phase and Oil As Modern Phase On The Disease Vyanga'Dokument8 SeitenPharmaceutical and Clinical Study of Kumkumadi Cream Prepared Using Kwath As Water Phase and Oil As Modern Phase On The Disease Vyanga'freemoronsNoch keine Bewertungen
- Spirituality, Spiritual Well-Being, and Spiritual Coping in Advanced Heart FailureDokument18 SeitenSpirituality, Spiritual Well-Being, and Spiritual Coping in Advanced Heart FailurezakiaNoch keine Bewertungen
- Circulatory System Review WorksheetDokument2 SeitenCirculatory System Review WorksheetCatherine JacksonNoch keine Bewertungen
- 8-Drugs Used in Anxiety and Panic Disprder (Edited)Dokument11 Seiten8-Drugs Used in Anxiety and Panic Disprder (Edited)ana01210761809Noch keine Bewertungen
- Comprehensive Review of Chest Tube Management A ReviewDokument6 SeitenComprehensive Review of Chest Tube Management A ReviewCesar LinaresNoch keine Bewertungen
- Workshop On Early Warning Score System - Ali HaedarDokument76 SeitenWorkshop On Early Warning Score System - Ali HaedarVicky ShuarNoch keine Bewertungen
- A Comprehensive Overview On Osteoporosis and Its Risk FactorsDokument21 SeitenA Comprehensive Overview On Osteoporosis and Its Risk Factorsdenta aeNoch keine Bewertungen
- Domiciliary Midwifery RDokument16 SeitenDomiciliary Midwifery Rswillymadhu83% (6)
- Changes in Diet and Lifestyle and Long-Term Weight Gain in Women and MenDokument13 SeitenChanges in Diet and Lifestyle and Long-Term Weight Gain in Women and MenemanvitoriaNoch keine Bewertungen
- Sterile Parenteral Products: A Narrative Approach: Journal of Drug Delivery and TherapeuticsDokument8 SeitenSterile Parenteral Products: A Narrative Approach: Journal of Drug Delivery and TherapeuticsArinta Purwi SuhartiNoch keine Bewertungen
- MCQ On 08.11.21Dokument2 SeitenMCQ On 08.11.21JENNIFER JOHN MBBS2020Noch keine Bewertungen
- Ob WARDDokument7 SeitenOb WARDNursingNooBNoch keine Bewertungen
- 2021 - Atosiban in Preterm Labor ManagementDokument45 Seiten2021 - Atosiban in Preterm Labor ManagementM Wahyu UtomoNoch keine Bewertungen
- TLE10 - 2nd Quarter Module 1Dokument5 SeitenTLE10 - 2nd Quarter Module 1VernaNoch keine Bewertungen
- Chapter 7. CirculationDokument54 SeitenChapter 7. CirculationankurbiologyNoch keine Bewertungen
- Inferior Vena Cava and Its TributariesDokument12 SeitenInferior Vena Cava and Its TributariesRahaf MajadlyNoch keine Bewertungen
- Diabetes Research and Clinical Practice: SciencedirectDokument2 SeitenDiabetes Research and Clinical Practice: Sciencedirectprobo asmoroNoch keine Bewertungen
- OPfr4 2Dokument13 SeitenOPfr4 26E Rivera Cervantes Osiris MargaritaNoch keine Bewertungen
- (Dental Discussion 1) - Hesy ReDokument32 Seiten(Dental Discussion 1) - Hesy ReethanNoch keine Bewertungen
- Effect of Full Crown Preparation On Pulpal Blood Flow in Man. Marisa Sukapattee. 2016. Archives of Oral BiologyDokument6 SeitenEffect of Full Crown Preparation On Pulpal Blood Flow in Man. Marisa Sukapattee. 2016. Archives of Oral BiologyValeria CrespoNoch keine Bewertungen
- Type 1 Diabetes MellitusDokument4 SeitenType 1 Diabetes MellitusLaura Lhoeste100% (1)
- Ncma: Health AssessmentDokument25 SeitenNcma: Health AssessmentBb PrintsNoch keine Bewertungen
- Intra OpDokument12 SeitenIntra OpalodiarkNoch keine Bewertungen
- Pneumonectomy S RT RpaDokument4 SeitenPneumonectomy S RT RpagireeshsachinNoch keine Bewertungen
- Management Guide Commercial Cage English Vs L0260-6Dokument88 SeitenManagement Guide Commercial Cage English Vs L0260-6Juliana de Souza Granja BarrosNoch keine Bewertungen
- Pancreatic Cancer - Case AnalysisDokument37 SeitenPancreatic Cancer - Case AnalysisMavy CantonNoch keine Bewertungen
- Bowel PreparationDokument20 SeitenBowel Preparationrosybash100% (1)
- D'OXYVA Information Summary For Healthcare Professionals - Proofreadv3 W.O CommentsDokument12 SeitenD'OXYVA Information Summary For Healthcare Professionals - Proofreadv3 W.O CommentsCircularity HealthcareNoch keine Bewertungen
- Uworld - PSYCHIATRYDokument24 SeitenUworld - PSYCHIATRYNikxyNoch keine Bewertungen