Das könnte Ihnen auch gefallen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Payanay Fatima May E. Bsn-2A // CHN LecDokument4 SeitenPayanay Fatima May E. Bsn-2A // CHN LecMarielle AcojidoNoch keine Bewertungen
- PDF 5 Steps To Give Her Screaming Hip Shaking Orgasms DLDokument24 SeitenPDF 5 Steps To Give Her Screaming Hip Shaking Orgasms DLosama abdoNoch keine Bewertungen
- Epilepsy in Pregnancy-IntroductionDokument9 SeitenEpilepsy in Pregnancy-Introductionfiraol mokonnenNoch keine Bewertungen
- Hypnobirthing - The Mongan Method - Is A Unique Method of Relaxed, NaturalDokument3 SeitenHypnobirthing - The Mongan Method - Is A Unique Method of Relaxed, NaturalZhaii Garcia MariacaNoch keine Bewertungen
- Final NCC Monograph Web-4!29!10Dokument20 SeitenFinal NCC Monograph Web-4!29!10nadaifilhoNoch keine Bewertungen
- Management of Diabetes in Pregnancy: Naveen Kumar MDokument12 SeitenManagement of Diabetes in Pregnancy: Naveen Kumar MNaveenKumarNoch keine Bewertungen
- Sambia: Papua New GuineaDokument11 SeitenSambia: Papua New GuineasandyNoch keine Bewertungen
- 7 Physiology of Normal Spontaneous Vaginal DeliveryDokument8 Seiten7 Physiology of Normal Spontaneous Vaginal DeliveryJohn Alfred GalarosaNoch keine Bewertungen
- Recommended Actions After Late or Missed Combined Oral ContraceptivesDokument2 SeitenRecommended Actions After Late or Missed Combined Oral ContraceptivesGreg100% (1)
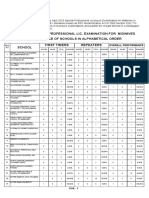
- April 2023 Special Professional Lic. Examination For MidwivesDokument2 SeitenApril 2023 Special Professional Lic. Examination For MidwivesRapplerNoch keine Bewertungen
- Lec-1) Different Terminology Used in ObstetricDokument14 SeitenLec-1) Different Terminology Used in ObstetricSaeed ShahNoch keine Bewertungen
- Postpartum HemorrhageDokument25 SeitenPostpartum HemorrhageaKmaL67% (3)
- Controversies in Family Planning: How To Manage A Fractured IUDDokument5 SeitenControversies in Family Planning: How To Manage A Fractured IUDPridina SyadirahNoch keine Bewertungen
- Alcohol 1Dokument4 SeitenAlcohol 1kasi metricsNoch keine Bewertungen
- Kant - Duties Toward The BodyDokument4 SeitenKant - Duties Toward The BodynobuyukiNoch keine Bewertungen
- 2 - PPT DR Liong Boy Kurniawan - Recent Update of Semen Analysis, LBK, KONAS 2022Dokument34 Seiten2 - PPT DR Liong Boy Kurniawan - Recent Update of Semen Analysis, LBK, KONAS 2022NANANoch keine Bewertungen
- Need For Sex Education For AdolescentsDokument25 SeitenNeed For Sex Education For AdolescentsAbharika SharmaNoch keine Bewertungen
- Q2 - 06 - Kinship, Marriage and HouseholdDokument37 SeitenQ2 - 06 - Kinship, Marriage and HouseholdHenry BuemioNoch keine Bewertungen
- Born This Way - Sexual Orientation Beliefs and Their Correlates...Dokument14 SeitenBorn This Way - Sexual Orientation Beliefs and Their Correlates...João Paulo Machado FeitozaNoch keine Bewertungen
- Uso de Miso en Obstetricia Ipas Mexico PDFDokument39 SeitenUso de Miso en Obstetricia Ipas Mexico PDFthedNoch keine Bewertungen
- Uself - Week 3 LessonDokument16 SeitenUself - Week 3 LessonAteng CrisNoch keine Bewertungen
- Legal Opinion For Tsi Ming ChoiDokument2 SeitenLegal Opinion For Tsi Ming ChoiJovan GasconNoch keine Bewertungen
- Human Sexuality CSL650 Reaction PaperDokument9 SeitenHuman Sexuality CSL650 Reaction PaperTe-Erika50% (2)
- Ob Final Exam GuideDokument30 SeitenOb Final Exam GuideSarah Elizabeth WalkerNoch keine Bewertungen
- (Libro) The Role of Biotechnology in Improvement of Livestock Animal Health and Biotechnology-Muhammad Abubakar, Ali Saeed, ODokument151 Seiten(Libro) The Role of Biotechnology in Improvement of Livestock Animal Health and Biotechnology-Muhammad Abubakar, Ali Saeed, OramsesmuseNoch keine Bewertungen
- Gender & Society (Phil)Dokument50 SeitenGender & Society (Phil)Maritoni MedallaNoch keine Bewertungen
- Gynae SNI Final Print VersionDokument34 SeitenGynae SNI Final Print VersionMr Soman Nadim IqbalNoch keine Bewertungen
- Chapter 5 - Letitia Richford - Cord ProlapseDokument6 SeitenChapter 5 - Letitia Richford - Cord ProlapseEunice Cortés100% (1)
- PatriarchyDokument1 SeitePatriarchyapi-374050745Noch keine Bewertungen
- Donnez 2012 - PEARL I PDFDokument12 SeitenDonnez 2012 - PEARL I PDFPaul B. WirawanNoch keine Bewertungen