Das könnte Ihnen auch gefallen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- DiseaseDokument15 SeitenDiseaseReymar HayNoch keine Bewertungen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (894)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Nursing considerations for Epoetin alfa (Eprex) administrationDokument2 SeitenNursing considerations for Epoetin alfa (Eprex) administrationIzell Lee100% (2)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Blood DopingDokument16 SeitenBlood Dopingpriyanka lalwaniNoch keine Bewertungen
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- Medicine MCQs For Medical Professionals - 3E (2013) (PDF)Dokument933 SeitenMedicine MCQs For Medical Professionals - 3E (2013) (PDF)Rohit Rajeev100% (14)
- Blood Cells, Immunity and Blood ClottingDokument65 SeitenBlood Cells, Immunity and Blood Clottingmunaamuummee100% (1)
- University of Al-Ameed College of Medicine: Hematopathology Lecture PlanDokument226 SeitenUniversity of Al-Ameed College of Medicine: Hematopathology Lecture PlanYousif AlaaNoch keine Bewertungen
- Blood & Blood ProductsDokument126 SeitenBlood & Blood ProductsdrprasadingleyNoch keine Bewertungen
- Cellular Regulation - Nursing Test QuestionsDokument124 SeitenCellular Regulation - Nursing Test QuestionsRNStudent1100% (2)
- Assessment of The Hematologic SystemDokument36 SeitenAssessment of The Hematologic SystemUSC Upstate Nursing CoachesNoch keine Bewertungen
- ToxoplasmosisDokument7 SeitenToxoplasmosisEgha Ratu EdoNoch keine Bewertungen
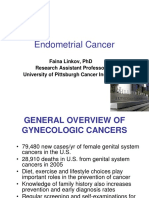
- Endometrial Cancer: Faina Linkov, PHD Research Assistant Professor University of Pittsburgh Cancer InstituteDokument22 SeitenEndometrial Cancer: Faina Linkov, PHD Research Assistant Professor University of Pittsburgh Cancer InstituteWenNy RupiNaNoch keine Bewertungen
- MR 2 Juni OA, AzotemiaDokument32 SeitenMR 2 Juni OA, AzotemiaWenNy RupiNaNoch keine Bewertungen
- 29 4 2011.Tn Samsi - stemI,.Shock, KADDokument23 Seiten29 4 2011.Tn Samsi - stemI,.Shock, KADWenNy RupiNaNoch keine Bewertungen
- Pallor and Weakness in 56 Year Old FemaleDokument12 SeitenPallor and Weakness in 56 Year Old FemaleWenNy RupiNaNoch keine Bewertungen
- AHA/ASA Guideline: Guidelines For The Early Management of Patients With Acute Ischemic StrokeDokument64 SeitenAHA/ASA Guideline: Guidelines For The Early Management of Patients With Acute Ischemic StrokeWenNy RupiNaNoch keine Bewertungen
- MR 6 Juni Tumor Paru, Azotemia Renal Dan Anemia NNDokument15 SeitenMR 6 Juni Tumor Paru, Azotemia Renal Dan Anemia NNWenNy RupiNaNoch keine Bewertungen
- Endometrial Cancer: Faina Linkov, PHD Research Assistant Professor University of Pittsburgh Cancer InstituteDokument22 SeitenEndometrial Cancer: Faina Linkov, PHD Research Assistant Professor University of Pittsburgh Cancer InstituteWenNy RupiNaNoch keine Bewertungen
- Morning Report 30 Mei Edit 2Dokument10 SeitenMorning Report 30 Mei Edit 2WenNy RupiNaNoch keine Bewertungen
- MR 20 May Sob Copd FixDokument30 SeitenMR 20 May Sob Copd FixWenNy RupiNaNoch keine Bewertungen
- UnicefDokument61 SeitenUnicefUgaugaaNoch keine Bewertungen
- UnicefDokument61 SeitenUnicefUgaugaaNoch keine Bewertungen
- Cerebral Palsy After Neonatal Encephalopathy PIIS0022347615001559 PDFDokument7 SeitenCerebral Palsy After Neonatal Encephalopathy PIIS0022347615001559 PDFWenNy RupiNaNoch keine Bewertungen
- Between-Hospital Variation in Treatment and Outcomes in Extremely Preterm InfantsDokument11 SeitenBetween-Hospital Variation in Treatment and Outcomes in Extremely Preterm InfantsAstri Faluna SheylavontiaNoch keine Bewertungen
- Which Biomarker Which Sepsis Neonatal Jurnal 2 PDFDokument8 SeitenWhich Biomarker Which Sepsis Neonatal Jurnal 2 PDFWenNy RupiNaNoch keine Bewertungen
- Systemic Review of Neonatal Seizure Management Strategies Provides Guidance On Anti Epileptic Treatment 4Dokument7 SeitenSystemic Review of Neonatal Seizure Management Strategies Provides Guidance On Anti Epileptic Treatment 4WenNy RupiNaNoch keine Bewertungen
- Pharmalogical Treatment of Neonatal Seizures A Systematic Review5Dokument19 SeitenPharmalogical Treatment of Neonatal Seizures A Systematic Review5WenNy RupiNaNoch keine Bewertungen
- In Vitro Plasmodium Falciparum Jurnal 4Dokument5 SeitenIn Vitro Plasmodium Falciparum Jurnal 4WenNy RupiNaNoch keine Bewertungen
- Which Biomarker Which Sepsis Neonatal Jurnal 2 PDFDokument8 SeitenWhich Biomarker Which Sepsis Neonatal Jurnal 2 PDFWenNy RupiNaNoch keine Bewertungen
- Pharmalogical Treatment of Neonatal Seizures A Systematic Review5Dokument19 SeitenPharmalogical Treatment of Neonatal Seizures A Systematic Review5WenNy RupiNaNoch keine Bewertungen
- Data Skripsi 2011Dokument18 SeitenData Skripsi 2011WenNy RupiNaNoch keine Bewertungen
- Erythropoiesis: Presented by DR Etu-Efeotor T. PDokument88 SeitenErythropoiesis: Presented by DR Etu-Efeotor T. PPrincewill SeiyefaNoch keine Bewertungen
- Antianemia Agents: Iron Vit B12 Folic Acid Copper Pyridoxine, RiboflavineDokument21 SeitenAntianemia Agents: Iron Vit B12 Folic Acid Copper Pyridoxine, RiboflavineRirin AfriantoNoch keine Bewertungen
- ErytHroCyte ProduCtionDokument8 SeitenErytHroCyte ProduCtionMichelle CaamicNoch keine Bewertungen
- Anemia Chronic DiseaseDokument51 SeitenAnemia Chronic Diseased_shadevNoch keine Bewertungen
- Blood Questions: (Total 5 Marks)Dokument11 SeitenBlood Questions: (Total 5 Marks)T-Jay Ellis-DaleNoch keine Bewertungen
- Anesthesia Analgesia September 2009Dokument291 SeitenAnesthesia Analgesia September 2009Alexandra PavloviciNoch keine Bewertungen
- Epoetin AlfaDokument3 SeitenEpoetin Alfaapi-3797941Noch keine Bewertungen
- 05 Polycythemia in The NewbornDokument11 Seiten05 Polycythemia in The NewbornMorales Eli PediatraNoch keine Bewertungen
- Erythropoiesis DPT SEM.1Dokument29 SeitenErythropoiesis DPT SEM.1Hifza KhanNoch keine Bewertungen
- Anemia and Chronic Kidney Disease: Stages 1-4Dokument16 SeitenAnemia and Chronic Kidney Disease: Stages 1-4Pearl Raiza HadaniNoch keine Bewertungen
- Hemoglobin Repo It inDokument1 SeiteHemoglobin Repo It inozamnNoch keine Bewertungen
- Anemia: Rheumatoid ArthritisDokument8 SeitenAnemia: Rheumatoid ArthritistyasNoch keine Bewertungen
- HaematinicsDokument20 SeitenHaematinicsGeetika Mehta100% (1)
- PolycythemiaDokument3 SeitenPolycythemiaSaraNoch keine Bewertungen
- Textbook of Veterinary Internal Medicine, 8th Edition-4693-4728 (1) - 1-18Dokument19 SeitenTextbook of Veterinary Internal Medicine, 8th Edition-4693-4728 (1) - 1-18Kevin Andres Trujillo CastroNoch keine Bewertungen
- Polycythemia Vera: What Are The Symptoms of Polycythemia?Dokument10 SeitenPolycythemia Vera: What Are The Symptoms of Polycythemia?Dimpal ChoudharyNoch keine Bewertungen
- Medical Oncology Jan2018Dokument64 SeitenMedical Oncology Jan2018Prajan JNoch keine Bewertungen
- Endocrinology of Genitourinary SystemDokument4 SeitenEndocrinology of Genitourinary SystemGerardLumNoch keine Bewertungen
- Hematology Must Knows PDFDokument34 SeitenHematology Must Knows PDFJeffrey LimNoch keine Bewertungen
- Pe11 q2 Mod2 Fitness-Enhancement-Through-SportsDokument32 SeitenPe11 q2 Mod2 Fitness-Enhancement-Through-SportsEugene ColotNoch keine Bewertungen
- Muhammad Adi Azfar Bin Rosli Muhammad Nazirul Fikri Bin Ahmad Rijaludin Nurshakila Binti SanisDokument23 SeitenMuhammad Adi Azfar Bin Rosli Muhammad Nazirul Fikri Bin Ahmad Rijaludin Nurshakila Binti Sanisnazki farNoch keine Bewertungen