Das könnte Ihnen auch gefallen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Nbme FlashcardsDokument150 SeitenNbme Flashcardsyasir saeed88% (8)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- DR - Ali UWORLD NOTESDokument1 SeiteDR - Ali UWORLD NOTESyasir saeedNoch keine Bewertungen
- HRBPDokument8 SeitenHRBPPriscilia KarinaNoch keine Bewertungen
- Filipino Catholic Wedding Ceremony LiturgyDokument8 SeitenFilipino Catholic Wedding Ceremony LiturgyHoney Joy ChuaNoch keine Bewertungen
- Ledger - Problems and SolutionsDokument1 SeiteLedger - Problems and SolutionsDjamal SalimNoch keine Bewertungen
- Metamath: A Computer Language For Mathematical ProofsDokument247 SeitenMetamath: A Computer Language For Mathematical ProofsJohn DoeNoch keine Bewertungen
- CS Blue Sheet Mnemonics - USMLE Step 2 CSDokument1 SeiteCS Blue Sheet Mnemonics - USMLE Step 2 CSyasir saeedNoch keine Bewertungen
- How To Prepare For InterviewDokument6 SeitenHow To Prepare For Interviewyasir saeedNoch keine Bewertungen
- Design Inducer PumpDokument2 SeitenDesign Inducer PumpnicoNoch keine Bewertungen
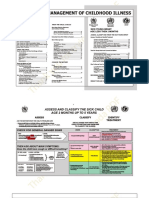
- IMNCI Chart Booklet (New) OrignalDokument36 SeitenIMNCI Chart Booklet (New) Orignalyasir saeedNoch keine Bewertungen
- Most Common CauseDokument9 SeitenMost Common CauseHemali KanabarNoch keine Bewertungen
- Cervical Cancer Screening StuffDokument3 SeitenCervical Cancer Screening Stuffyasir saeedNoch keine Bewertungen
- Step 2 Cs CasesDokument4 SeitenStep 2 Cs Casesyasir saeedNoch keine Bewertungen
- Step 2 Cs CasesDokument4 SeitenStep 2 Cs Casesyasir saeedNoch keine Bewertungen
- Uworld NotesDokument1 SeiteUworld Notesyasir saeedNoch keine Bewertungen
- Taking History in MedicineDokument17 SeitenTaking History in Medicineyasir saeed100% (1)
- Test For 4th (Trochlear) Nerve PalsyDokument23 SeitenTest For 4th (Trochlear) Nerve Palsyyasir saeedNoch keine Bewertungen
- Wet Specimen Preservation MethodsDokument24 SeitenWet Specimen Preservation Methodstamil selvanNoch keine Bewertungen
- UI Symphony Orchestra and Choirs Concert Features Mahler's ResurrectionDokument17 SeitenUI Symphony Orchestra and Choirs Concert Features Mahler's ResurrectionJilly CookeNoch keine Bewertungen
- Trends1 Aio TT2-L2Dokument4 SeitenTrends1 Aio TT2-L2Bart Simpsons FernándezNoch keine Bewertungen
- Alcatel 350 User Guide FeaturesDokument4 SeitenAlcatel 350 User Guide FeaturesFilipe CardosoNoch keine Bewertungen
- CHAPTER 8 SULLIVAN MyReviewerDokument7 SeitenCHAPTER 8 SULLIVAN MyReviewerFrances LouiseNoch keine Bewertungen
- Clare Redman Statement of IntentDokument4 SeitenClare Redman Statement of Intentapi-309923259Noch keine Bewertungen
- The Message Development Tool - A Case For Effective Operationalization of Messaging in Social Marketing PracticeDokument17 SeitenThe Message Development Tool - A Case For Effective Operationalization of Messaging in Social Marketing PracticesanjayamalakasenevirathneNoch keine Bewertungen
- AmpConectorsExtracto PDFDokument5 SeitenAmpConectorsExtracto PDFAdrian AvilesNoch keine Bewertungen
- Dada and Buddhist Thought - Sung-Won Ko PDFDokument24 SeitenDada and Buddhist Thought - Sung-Won Ko PDFJuan Manuel Gomez GarcíaNoch keine Bewertungen
- Tauros TBM Guidance SystemDokument3 SeitenTauros TBM Guidance SystemMiloš StanimirovićNoch keine Bewertungen
- DP4XXX PricesDokument78 SeitenDP4XXX PricesWassim KaissouniNoch keine Bewertungen
- Ozone Layer EssayDokument7 SeitenOzone Layer Essayb71bpjha100% (2)
- 1 (Speaking of A Letter) I Made This One Longer, Only Because I Had Not Enough Time To Make It ShorterDokument10 Seiten1 (Speaking of A Letter) I Made This One Longer, Only Because I Had Not Enough Time To Make It ShorterJhancarlos Carrasco MNoch keine Bewertungen
- DHRM 3 SyllabusDokument10 SeitenDHRM 3 SyllabusCherokee Tuazon RodriguezNoch keine Bewertungen
- Lala Hardayal - BiographyDokument6 SeitenLala Hardayal - Biographyamarsingh1001Noch keine Bewertungen
- How Ventilators Deliver BreathsDokument51 SeitenHow Ventilators Deliver BreathsArnaldo SantizoNoch keine Bewertungen
- Material For Werable AntennaDokument4 SeitenMaterial For Werable AntennaMujeeb AbdullahNoch keine Bewertungen
- Neural Networks in Data Mining: Ripundeep Singh Gill, AshimaDokument6 SeitenNeural Networks in Data Mining: Ripundeep Singh Gill, AshimaIOSRJEN : hard copy, certificates, Call for Papers 2013, publishing of journalNoch keine Bewertungen
- INDIAMART 25012022003631 Investor Presentation Q3FY2021-22Dokument84 SeitenINDIAMART 25012022003631 Investor Presentation Q3FY2021-22geethvazNoch keine Bewertungen
- Sample Management Representation Letter Type II SAS 70 AuditDokument2 SeitenSample Management Representation Letter Type II SAS 70 Auditaaldawi0% (1)
- WEEK 1 Materi-EM101-M01-The Foundation of Business 2Dokument48 SeitenWEEK 1 Materi-EM101-M01-The Foundation of Business 2ddhani299Noch keine Bewertungen
- Corporate Social Responsibility International PerspectivesDokument14 SeitenCorporate Social Responsibility International PerspectivesR16094101李宜樺Noch keine Bewertungen
- Turning Frequency in Adult Bedridden Patients To Prevent Hospital-Acquired Pressure Ulcer: A Scoping ReviewDokument12 SeitenTurning Frequency in Adult Bedridden Patients To Prevent Hospital-Acquired Pressure Ulcer: A Scoping ReviewfajaqaNoch keine Bewertungen
- National Artists of the PhilippinesDokument66 SeitenNational Artists of the Philippinesshey mahilumNoch keine Bewertungen
- Chartered Accountants and Accountans in AmbalaDokument3 SeitenChartered Accountants and Accountans in AmbalaGurmeet kaurNoch keine Bewertungen