Das könnte Ihnen auch gefallen
- Evaporative Condenser Engineering Manual: Technical ResourcesDokument18 SeitenEvaporative Condenser Engineering Manual: Technical ResourcesMohamed IbrahimNoch keine Bewertungen
- Expansion Tank Design Guide, How To Size and Select An Expansion Tank For A Chilled Water System 3Dokument1 SeiteExpansion Tank Design Guide, How To Size and Select An Expansion Tank For A Chilled Water System 3CunCunAlAndraNoch keine Bewertungen
- Evaporative Condenser Engineering Manual: Technical ResourcesDokument18 SeitenEvaporative Condenser Engineering Manual: Technical ResourcesMohamed IbrahimNoch keine Bewertungen
- Expansion Tank Design Guide, How To Size and Select An Expansion Tank For A Chilled Water System 1Dokument1 SeiteExpansion Tank Design Guide, How To Size and Select An Expansion Tank For A Chilled Water System 1CunCunAlAndraNoch keine Bewertungen
- Evaporative Condenser Engineering Manual: Technical ResourcesDokument18 SeitenEvaporative Condenser Engineering Manual: Technical ResourcesMohamed IbrahimNoch keine Bewertungen
- Expansion Tank Design Guide, How To Size and Select An Expansion Tank For A Chilled Water System 2Dokument1 SeiteExpansion Tank Design Guide, How To Size and Select An Expansion Tank For A Chilled Water System 2CunCunAlAndraNoch keine Bewertungen
- Management Gathering 0718 - Distribution - v5 CoverDokument1 SeiteManagement Gathering 0718 - Distribution - v5 CoverCunCunAlAndraNoch keine Bewertungen
- Consulting Business ModelDokument1 SeiteConsulting Business ModelCunCunAlAndraNoch keine Bewertungen
- Process Plant Layout - Seán Moran 3-4Dokument2 SeitenProcess Plant Layout - Seán Moran 3-4CunCunAlAndraNoch keine Bewertungen
- GF Signet 515 2536 Manual02Dokument1 SeiteGF Signet 515 2536 Manual02CunCunAlAndraNoch keine Bewertungen
- DA38 Safety Data Shett FAME (Fatty Acid Methyl Ester) V4 - en - DEDokument14 SeitenDA38 Safety Data Shett FAME (Fatty Acid Methyl Ester) V4 - en - DECunCunAlAndraNoch keine Bewertungen
- RicoDokument62 SeitenRicoCunCunAlAndraNoch keine Bewertungen
- Process Plant Layout - Seán Moran 1-2Dokument2 SeitenProcess Plant Layout - Seán Moran 1-2CunCunAlAndra100% (1)
- GF Signet 515 2536 Manual01Dokument1 SeiteGF Signet 515 2536 Manual01CunCunAlAndraNoch keine Bewertungen
- RCOG Guidelines - Gestational Trophoblastic DiseaseDokument12 SeitenRCOG Guidelines - Gestational Trophoblastic Diseasemob3100% (1)
- 1348493956.2409obstetrics Handbook PDFDokument48 Seiten1348493956.2409obstetrics Handbook PDFdrng48Noch keine Bewertungen
- Frontline Gastroenterol 2014 Dyson Flgastro 2013 100404Dokument11 SeitenFrontline Gastroenterol 2014 Dyson Flgastro 2013 100404CunCunAlAndraNoch keine Bewertungen
- Gastro Enter Oh Epa ToDokument29 SeitenGastro Enter Oh Epa TodeliaintanNoch keine Bewertungen
- Early Liver TransplantationDokument11 SeitenEarly Liver TransplantationCunCunAlAndraNoch keine Bewertungen
- NonalcoholicFattyLiverDisease2012 25762 FTPDokument19 SeitenNonalcoholicFattyLiverDisease2012 25762 FTPbudi_26690Noch keine Bewertungen
- RicoDokument62 SeitenRicoCunCunAlAndraNoch keine Bewertungen
- Problem 5 Git: Ivan MichaelDokument68 SeitenProblem 5 Git: Ivan MichaelCunCunAlAndraNoch keine Bewertungen
- Kjae-68-101 Transfusion-Related Acute Lung InjuryDokument5 SeitenKjae-68-101 Transfusion-Related Acute Lung InjuryCunCunAlAndraNoch keine Bewertungen
- RCOG Guidelines - Gestational Trophoblastic DiseaseDokument12 SeitenRCOG Guidelines - Gestational Trophoblastic Diseasemob3100% (1)
- Pitri - GI.Pemicu 4. GE+ Tifus AbdominalisDokument154 SeitenPitri - GI.Pemicu 4. GE+ Tifus AbdominalisCunCunAlAndraNoch keine Bewertungen
- MAPAX1Dokument2 SeitenMAPAX1CunCunAlAndraNoch keine Bewertungen
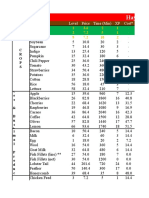
- Hay Day Price Profit AnalysisDokument112 SeitenHay Day Price Profit AnalysisCunCunAlAndraNoch keine Bewertungen
- Hay Day Price Profit AnalysisDokument112 SeitenHay Day Price Profit AnalysisCunCunAlAndraNoch keine Bewertungen
- Hay Day Price Profit AnalysisDokument112 SeitenHay Day Price Profit AnalysisCunCunAlAndraNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (120)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- 12th Ed Twenty Questions FaqDokument6 Seiten12th Ed Twenty Questions FaqpatriciaNoch keine Bewertungen
- DST Final Exam NotesDokument56 SeitenDST Final Exam NoteslmaoheartsNoch keine Bewertungen
- BP Open Sampling & Additivisation Procedure 1 - 0Dokument51 SeitenBP Open Sampling & Additivisation Procedure 1 - 0ParaZzzitNoch keine Bewertungen
- Emotional BarometerDokument1 SeiteEmotional BarometerAshok JNoch keine Bewertungen
- Professional Learning Record Chart YrDokument11 SeitenProfessional Learning Record Chart Yrapi-716050560Noch keine Bewertungen
- Chapter 25Dokument27 SeitenChapter 25Kriana RosalesNoch keine Bewertungen
- Pre - Registration Log BookDokument14 SeitenPre - Registration Log BooksimbaiNoch keine Bewertungen
- Counseling - Its Principles, MethodsDokument36 SeitenCounseling - Its Principles, MethodsCarmz PeraltaNoch keine Bewertungen
- UNDERSTANDING THE SELF ModuleDokument57 SeitenUNDERSTANDING THE SELF ModuleNaga View100% (5)
- Hijama Cupping PDFDokument16 SeitenHijama Cupping PDFMuhammad Khalid JavedNoch keine Bewertungen
- Idb TemplateDokument5 SeitenIdb TemplatePrinces Vench SanchezNoch keine Bewertungen
- HRM PPT 1Dokument49 SeitenHRM PPT 1jade.salvadoNoch keine Bewertungen
- 108 Answer KeyDokument4 Seiten108 Answer KeyKryzza LeizellNoch keine Bewertungen
- First Periodical Mapeh 9Dokument5 SeitenFirst Periodical Mapeh 9Juvy Singian100% (1)
- West Philippine SeaDokument4 SeitenWest Philippine SeaFrancheskalane ValenciaNoch keine Bewertungen
- Evaluation of Scientific Publications - Part 22 - Estimation of Effects in The Absence of Head-to-Head Trials PDFDokument6 SeitenEvaluation of Scientific Publications - Part 22 - Estimation of Effects in The Absence of Head-to-Head Trials PDFPhoNoch keine Bewertungen
- The PACE Trial: Radiotherapy Planning and Delivery Guidelines (Pace-A and Pace-C)Dokument33 SeitenThe PACE Trial: Radiotherapy Planning and Delivery Guidelines (Pace-A and Pace-C)Анастасия АнохинаNoch keine Bewertungen
- Edwards Lifescience Vigileo CatalogoDokument40 SeitenEdwards Lifescience Vigileo CatalogoDeni Leonardo TorresNoch keine Bewertungen
- 2017 STP Paed Neonates PDFDokument258 Seiten2017 STP Paed Neonates PDFChoden JamyangNoch keine Bewertungen
- COWELL Implant Solution v28Dokument146 SeitenCOWELL Implant Solution v28Julian MachoNoch keine Bewertungen
- First Quarter Examination Mapeh 8: Raba National High SchoolDokument2 SeitenFirst Quarter Examination Mapeh 8: Raba National High SchoolJay50% (4)
- Practical Guideline in Office Hysteroscopy SEGiDokument95 SeitenPractical Guideline in Office Hysteroscopy SEGiMarcus MenezesNoch keine Bewertungen
- Oral and Naso Pharyngeal SuctioningDokument10 SeitenOral and Naso Pharyngeal SuctioningMa. Ferimi Gleam BajadoNoch keine Bewertungen
- DR Saiful's Notes On Medical - Allied Health Education - Curriculum Planning - DevelopmentDokument71 SeitenDR Saiful's Notes On Medical - Allied Health Education - Curriculum Planning - DevelopmentAdrest S MamuroNoch keine Bewertungen
- Ges New Jhs Syllabus Career Technology CCP Curriculum For b7 b10 Draft ZeroDokument367 SeitenGes New Jhs Syllabus Career Technology CCP Curriculum For b7 b10 Draft ZeroElvis Adjei Yamoah100% (1)
- Discharge PlanDokument9 SeitenDischarge PlanRheynel NietesNoch keine Bewertungen
- Y.E.S.-student's Feedback FormDokument2 SeitenY.E.S.-student's Feedback FormSneha Kothawade - Awaken YogNoch keine Bewertungen
- Mendoza Jose David B. Module 6Dokument5 SeitenMendoza Jose David B. Module 6chlspat12Noch keine Bewertungen
- Test Bank For Oral Pathology For The Dental Hygienist 7th Edition by IbsenDokument36 SeitenTest Bank For Oral Pathology For The Dental Hygienist 7th Edition by Ibsenknurtailrace.k90riy100% (39)
- Project Report On Hospital - 100 BedsDokument3 SeitenProject Report On Hospital - 100 BedsEIRI Board of Consultants and Publishers100% (1)