Das könnte Ihnen auch gefallen
- Primary Survey & Secondary Survey: Presentor: Shellazianne Anak Ringam Date: 20 November 2015Dokument27 SeitenPrimary Survey & Secondary Survey: Presentor: Shellazianne Anak Ringam Date: 20 November 2015Keluang Man WinchesterNoch keine Bewertungen
- Airway AdjunctsDokument17 SeitenAirway AdjunctsChannelGNoch keine Bewertungen
- Emergency Case Review: Advanced Cardiac Life Support (ACLS) 2015Dokument51 SeitenEmergency Case Review: Advanced Cardiac Life Support (ACLS) 2015Lely Yuniarti AhqafNoch keine Bewertungen
- Secondary SurveyDokument18 SeitenSecondary SurveyJohn BrittoNoch keine Bewertungen
- Basic Principles of Trauma ManagementDokument53 SeitenBasic Principles of Trauma ManagementMohamed Saeed BachooNoch keine Bewertungen
- Anal FissuraDokument14 SeitenAnal FissuraAnonymous LoQcj2xENoch keine Bewertungen
- Formulari Ubat KKM 3/2012Dokument238 SeitenFormulari Ubat KKM 3/2012afiq83100% (3)
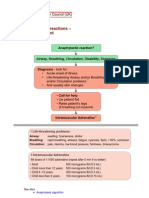
- Resuscitation Council Uk Anaphylaxis AlgorithmDokument1 SeiteResuscitation Council Uk Anaphylaxis Algorithmbrianed231100% (1)
- Insiden Bunuh Diri Secara Gantung DiriDokument8 SeitenInsiden Bunuh Diri Secara Gantung Diribellezaini.94Noch keine Bewertungen
- Head Trauma TreatmentDokument11 SeitenHead Trauma TreatmentIrmada Bohea IRNoch keine Bewertungen
- Chest Pain Non TraumaDokument45 SeitenChest Pain Non TraumaTita LuthfiaNoch keine Bewertungen
- Pediatric Head InjuryDokument9 SeitenPediatric Head InjuryAndy WijayaNoch keine Bewertungen
- Airway Obstruction - Types, Causes, and SymptomsDokument6 SeitenAirway Obstruction - Types, Causes, and SymptomsGilbertLiem100% (1)
- General ExaminationDokument112 SeitenGeneral ExaminationChiranjeevi Kumar EndukuruNoch keine Bewertungen
- Managment of Trauma Patient in ERDokument46 SeitenManagment of Trauma Patient in ERtofanNoch keine Bewertungen
- Blood Supply of External EarDokument4 SeitenBlood Supply of External EarSari Rahmawati Tajudin100% (1)
- Breath Holding SpellDokument3 SeitenBreath Holding SpellDimas Alphiano100% (1)
- Chapter 3 Airway Management in Trauma PatientDokument53 SeitenChapter 3 Airway Management in Trauma PatientMGCNoch keine Bewertungen
- Pain Management F05Dokument19 SeitenPain Management F05Aneka DeanNoch keine Bewertungen
- Approach To Interstitial Lung DiseasesDokument38 SeitenApproach To Interstitial Lung DiseasesmeawchiNoch keine Bewertungen
- Hyperglycemic Hyperosmolar StateDokument17 SeitenHyperglycemic Hyperosmolar StateAqila Mumtaz50% (2)
- 1 Early Management of Trauma Patient in The HospitalDokument23 Seiten1 Early Management of Trauma Patient in The HospitalkgnmatinNoch keine Bewertungen
- Kes StudyDokument17 SeitenKes StudyMellCy L'sNoch keine Bewertungen
- Case Report 2Dokument7 SeitenCase Report 2sofiosNoch keine Bewertungen
- Management of Local Anaesthetic Toxicity Update 2009Dokument6 SeitenManagement of Local Anaesthetic Toxicity Update 2009leviosagalNoch keine Bewertungen
- Pre Hospital Care in Malaysia - Issues and ChallengesDokument50 SeitenPre Hospital Care in Malaysia - Issues and Challengeschat5619100% (1)
- Tension PneumothoraxDokument18 SeitenTension PneumothoraxmeviraNoch keine Bewertungen
- Anaphylaxis Shock: Bagian Anestesi FK UNISSULA SemarangDokument15 SeitenAnaphylaxis Shock: Bagian Anestesi FK UNISSULA SemarangTeguh PambudiNoch keine Bewertungen
- Triage ZoneDokument4 SeitenTriage ZoneHafiz Hamidi100% (1)
- Dyspnea PresentationDokument37 SeitenDyspnea PresentationamgoperaNoch keine Bewertungen
- DyspneaDokument34 SeitenDyspneagiogoriNoch keine Bewertungen
- Anaesthesia For The Obese Obstetric PatientDokument85 SeitenAnaesthesia For The Obese Obstetric PatientDr.Deb Sanjay Nag100% (1)
- Constrictive Pericarditis - UpToDateDokument26 SeitenConstrictive Pericarditis - UpToDateSebastian CastañedaNoch keine Bewertungen
- Kelantan Guidelines For Nsteacs 2nd Edition 2012 PDFDokument48 SeitenKelantan Guidelines For Nsteacs 2nd Edition 2012 PDFAhmad Nafais RahimiNoch keine Bewertungen
- Preparing For The Prescribing Safety AssessmentDokument36 SeitenPreparing For The Prescribing Safety AssessmentChAndrewNoch keine Bewertungen
- Cataract InformationDokument25 SeitenCataract Informationvasanth_1515Noch keine Bewertungen
- ThyroidDokument13 SeitenThyroidczarmaine29Noch keine Bewertungen
- Amc Drug Study SimplifiedDokument2 SeitenAmc Drug Study Simplifiedtimie_reyesNoch keine Bewertungen
- Transport of Critically Ill PatientDokument26 SeitenTransport of Critically Ill PatientHayatul AkmaLia0% (1)
- Burn ManagementDokument64 SeitenBurn Managementabdullah100% (1)
- Early Assessment of Trauma Patients and ATLSDokument45 SeitenEarly Assessment of Trauma Patients and ATLSTILAHUNNoch keine Bewertungen
- Nice Guidelines For VteDokument512 SeitenNice Guidelines For VtesilcmtgNoch keine Bewertungen
- Derma Case Write UpDokument9 SeitenDerma Case Write UpAmbhi GanaNoch keine Bewertungen
- Anaphylaxis CEACCP 2004Dokument3 SeitenAnaphylaxis CEACCP 2004kuruppukarlNoch keine Bewertungen
- Muscle RelaxantDokument35 SeitenMuscle RelaxantwakwawNoch keine Bewertungen
- Cranial NervesDokument67 SeitenCranial NervesBahaa ShaabanNoch keine Bewertungen
- General Clerking in Orthopaedics House Officers Workshop MalaysiaDokument10 SeitenGeneral Clerking in Orthopaedics House Officers Workshop MalaysiaUzair MuhdNoch keine Bewertungen
- Nasal Septal Disorders: Dr. Omwenga Cliffe Facilitator: Dr. KipingorDokument45 SeitenNasal Septal Disorders: Dr. Omwenga Cliffe Facilitator: Dr. KipingorjustofitsNoch keine Bewertungen
- Snake Bite Medical ManagementDokument35 SeitenSnake Bite Medical Managementsyarifah nurlailaNoch keine Bewertungen
- Difficult IntubationDokument28 SeitenDifficult IntubationVG FernandezNoch keine Bewertungen
- Disaster and Multi-Casualty Triage: DR - Ramanujam.S Assistant Proffesor CareDokument96 SeitenDisaster and Multi-Casualty Triage: DR - Ramanujam.S Assistant Proffesor CareRamanujamNoch keine Bewertungen
- Polytrauma EARLY MX 2009Dokument87 SeitenPolytrauma EARLY MX 2009Fina Syafinaz SuhaimiNoch keine Bewertungen
- Trauma and Emergency NursingDokument9 SeitenTrauma and Emergency Nursingchinthaka18389021Noch keine Bewertungen
- Approach To Trauma PatientDokument36 SeitenApproach To Trauma PatientTitusNoch keine Bewertungen
- NYSORA Hazdics RegionalDokument8 SeitenNYSORA Hazdics RegionalAishu BNoch keine Bewertungen
- Advanced Trauma and Life Support (ATLS) : EpidemiologyDokument7 SeitenAdvanced Trauma and Life Support (ATLS) : EpidemiologyMohamed FarahatNoch keine Bewertungen
- Traum ManagementDokument7 SeitenTraum Managementchinthaka18389021Noch keine Bewertungen
- Approach To Trauma PatientDokument49 SeitenApproach To Trauma PatientHadinur Jufri100% (1)
- Dzino's SurgeryDokument718 SeitenDzino's SurgeryHuram SeremaniNoch keine Bewertungen
- Advances in Understanding The Pathogenesis of HLH: ReviewDokument14 SeitenAdvances in Understanding The Pathogenesis of HLH: Reviewizwan taufikNoch keine Bewertungen
- KoreAnesthesia 2020 - 추계연수강좌 강의록 - 최종 PDFDokument36 SeitenKoreAnesthesia 2020 - 추계연수강좌 강의록 - 최종 PDFizwan taufikNoch keine Bewertungen
- Eposters Abstract Form Congress 2021Dokument2 SeitenEposters Abstract Form Congress 2021izwan taufikNoch keine Bewertungen
- Total Revision For The Primary Frca 2nd EditionDokument53 SeitenTotal Revision For The Primary Frca 2nd Editionizwan taufikNoch keine Bewertungen
- Airway Adjunct and Difficult AirwayDokument19 SeitenAirway Adjunct and Difficult Airwayizwan taufikNoch keine Bewertungen
- CPG Early Management of Head Injury in AdultsDokument84 SeitenCPG Early Management of Head Injury in Adultsizwan taufikNoch keine Bewertungen
- Surgery Notes: For The M.B.B.S. by Andre TanDokument163 SeitenSurgery Notes: For The M.B.B.S. by Andre Tanizwan taufikNoch keine Bewertungen
- Sample CVDokument3 SeitenSample CVsam_mad00Noch keine Bewertungen
- Prayer Points 7 Day Prayer Fasting PerfectionDokument4 SeitenPrayer Points 7 Day Prayer Fasting PerfectionBenjamin Adelwini Bugri100% (6)
- Spare Parts Documentation: TD10004553 EN 00Dokument69 SeitenSpare Parts Documentation: TD10004553 EN 00Emon Sharma100% (1)
- All About Me - RubricDokument3 SeitenAll About Me - Rubricapi-314921155Noch keine Bewertungen
- Warcraft III ManualDokument47 SeitenWarcraft III Manualtrevorbourget78486100% (6)
- Direct Method (Education) : Navigation SearchDokument5 SeitenDirect Method (Education) : Navigation Searcheisha_91Noch keine Bewertungen
- 1 Hot Metal Tapping SOPDokument25 Seiten1 Hot Metal Tapping SOPSANJAY KUMAR PATINoch keine Bewertungen
- Violin Teaching in The New Millennium or Remembering The Future of Violin Performance by Gwendolyn Masin For Trinity College 2012Dokument241 SeitenViolin Teaching in The New Millennium or Remembering The Future of Violin Performance by Gwendolyn Masin For Trinity College 2012Matheus Felipe Lessa Oliveira100% (4)
- Windows Server Failover Clustering On HPE SimpliVity Technical White Paper-A50000833enwDokument15 SeitenWindows Server Failover Clustering On HPE SimpliVity Technical White Paper-A50000833enwYeraldo MarinNoch keine Bewertungen
- Geometry Unit: Congruence and Similarity: Manasquan High School Department: MathematicsDokument5 SeitenGeometry Unit: Congruence and Similarity: Manasquan High School Department: MathematicsabilodeauNoch keine Bewertungen
- Working Capital Management by Birla GroupDokument39 SeitenWorking Capital Management by Birla GroupHajra ShahNoch keine Bewertungen
- Alternate History of The WorldDokument2 SeitenAlternate History of The WorldCamille Ann Faigao FamisanNoch keine Bewertungen
- Micro Analysis Report - Int1Dokument3 SeitenMicro Analysis Report - Int1kousikkumaarNoch keine Bewertungen
- WLP Math Week 4 Q4Dokument4 SeitenWLP Math Week 4 Q4JUDELYN O. DOMINGONoch keine Bewertungen
- Frugal Innovation in Developed Markets - Adaption o - 2020 - Journal of InnovatiDokument9 SeitenFrugal Innovation in Developed Markets - Adaption o - 2020 - Journal of InnovatiGisselle RomeroNoch keine Bewertungen
- Formulating Affective Learning Targets: Category Examples and KeywordsDokument2 SeitenFormulating Affective Learning Targets: Category Examples and KeywordsJean LabradorNoch keine Bewertungen
- The Anti Cancer Essential Oil ReferenceDokument9 SeitenThe Anti Cancer Essential Oil ReferenceΡαφαέλα ΠηλείδηNoch keine Bewertungen
- 2014 Price ListDokument17 Seiten2014 Price ListMartin J.Noch keine Bewertungen
- Unit 4 Classical and Keynesian Systems: 4.0 ObjectivesDokument28 SeitenUnit 4 Classical and Keynesian Systems: 4.0 ObjectivesHemant KumarNoch keine Bewertungen
- Short Questions From 'The World Is Too Much With Us' by WordsworthDokument2 SeitenShort Questions From 'The World Is Too Much With Us' by WordsworthTANBIR RAHAMANNoch keine Bewertungen
- Student Skeletal System Exam QuestionsDokument3 SeitenStudent Skeletal System Exam Questionsawiniemmanuel247Noch keine Bewertungen
- Stoke Rehabilitation NICE GuidelinesDokument591 SeitenStoke Rehabilitation NICE GuidelinesHardeep Singh BaliNoch keine Bewertungen
- Nail DisordersDokument123 SeitenNail DisordersyaraamadoNoch keine Bewertungen
- Sow English Year 4 2023 2024Dokument12 SeitenSow English Year 4 2023 2024Shamien ShaNoch keine Bewertungen
- Assignment On How To Increase Own Brand Mantras: Submition Date: January 29,2021Dokument5 SeitenAssignment On How To Increase Own Brand Mantras: Submition Date: January 29,2021Ferari DroboNoch keine Bewertungen
- Applied Chemistry-IDokument16 SeitenApplied Chemistry-Islm.sbipNoch keine Bewertungen
- Revalida ResearchDokument3 SeitenRevalida ResearchJakie UbinaNoch keine Bewertungen
- Tectos Falsos Stretch Caracteristicas TecnicasDokument37 SeitenTectos Falsos Stretch Caracteristicas TecnicasVadymNoch keine Bewertungen
- Construction Skills Learning ExerciseDokument16 SeitenConstruction Skills Learning ExerciseAljaniaNoch keine Bewertungen
- Mapua Cwtsstudentsmodule (Ay08 09)Dokument62 SeitenMapua Cwtsstudentsmodule (Ay08 09)anon-805332Noch keine Bewertungen