Das könnte Ihnen auch gefallen
- Ch. 4 Critical Thinking ActivityDokument8 SeitenCh. 4 Critical Thinking ActivityYe YusiNoch keine Bewertungen
- 37 Warning Signs of RelapseDokument6 Seiten37 Warning Signs of Relapseryanh1904100% (2)
- Daftar Dosis Dan Sediaan Obat Untuk AnakDokument4 SeitenDaftar Dosis Dan Sediaan Obat Untuk AnakFitri Sutrisno87% (30)
- Yoli Acidity ReportDokument8 SeitenYoli Acidity ReportTroy Dooly100% (1)
- Sleep DisordersDokument49 SeitenSleep DisordersShivam SoniNoch keine Bewertungen
- Sleep-Wake DisordersDokument14 SeitenSleep-Wake Disordersnathanielge19Noch keine Bewertungen
- Narcolepsy and CataplexyDokument6 SeitenNarcolepsy and CataplexyAh BoonNoch keine Bewertungen
- Sleep DisordersDokument45 SeitenSleep DisordersOse IbhadodeNoch keine Bewertungen
- Sleep DisordersDokument23 SeitenSleep DisordersBEA RADANoch keine Bewertungen
- CCNDokument39 SeitenCCNMann TSha100% (1)
- Insomnia: Case Studies in Family Practice: Kamil Mohd Ariff Zailinawati Abu Hassan Author Information PMC DisclaimerDokument12 SeitenInsomnia: Case Studies in Family Practice: Kamil Mohd Ariff Zailinawati Abu Hassan Author Information PMC DisclaimerAbhishek AgrawalNoch keine Bewertungen
- Insomnia and HypersomnolenceDokument9 SeitenInsomnia and HypersomnolenceLABADAN, JOHANNA ALAINE S. 3-2Noch keine Bewertungen
- Sleep Disorders: By: Olivia B. Cantos Cherilyn C. CapunoDokument19 SeitenSleep Disorders: By: Olivia B. Cantos Cherilyn C. CapunoOlive CantosNoch keine Bewertungen
- Sleep Disorders-2Dokument13 SeitenSleep Disorders-2Hiba MohammedNoch keine Bewertungen
- Sleep DisordersDokument32 SeitenSleep DisordersRohini Selvarajah100% (1)
- Sleep DisordersDokument20 SeitenSleep DisordersKathleen Ellize BetchaydaNoch keine Bewertungen
- Sleep DisorderDokument9 SeitenSleep DisorderRanjan DasNoch keine Bewertungen
- Sleep Disorders: Review Neurology Series Editor, William J. Mullally, MDDokument8 SeitenSleep Disorders: Review Neurology Series Editor, William J. Mullally, MDniNoch keine Bewertungen
- Lewis: Medical-Surgical Nursing, 10 Edition: Sleep and Sleep Disorders Key Points SleepDokument4 SeitenLewis: Medical-Surgical Nursing, 10 Edition: Sleep and Sleep Disorders Key Points Sleepsophia onu100% (2)
- Treatment of Insomnia: An Alternative Approach: Anoja S. Attele, DDS, Jing-Tian Xie, MD, and Chun-Su Yuan, MD, PHDDokument11 SeitenTreatment of Insomnia: An Alternative Approach: Anoja S. Attele, DDS, Jing-Tian Xie, MD, and Chun-Su Yuan, MD, PHDimamlutfi13Noch keine Bewertungen
- Pharmacology 2Dokument37 SeitenPharmacology 2jekeri bekeriNoch keine Bewertungen
- Sleep Wake DisordersDokument5 SeitenSleep Wake DisordersIsabel CastilloNoch keine Bewertungen
- Sleep-Wake DisordersDokument61 SeitenSleep-Wake Disorderskume senbetaNoch keine Bewertungen
- Day 9 ASSIGNMENT SDDokument3 SeitenDay 9 ASSIGNMENT SDashwinNoch keine Bewertungen
- Narcolepsy, A Simple Guide to the Condition, Treatment and Related DiseasesVon EverandNarcolepsy, A Simple Guide to the Condition, Treatment and Related DiseasesBewertung: 1 von 5 Sternen1/5 (2)
- Sleep Disorders: Its Causes and TreatmentsDokument20 SeitenSleep Disorders: Its Causes and TreatmentsBasari OdalNoch keine Bewertungen
- Sleep DisordersDokument5 SeitenSleep DisorderssookoojessicaNoch keine Bewertungen
- Nursing Care Plan For InsomiaDokument4 SeitenNursing Care Plan For InsomiaLord Pozak MillerNoch keine Bewertungen
- CCJM Advances in Treating InsomniaDokument11 SeitenCCJM Advances in Treating InsomniaBrian HarrisNoch keine Bewertungen
- Sleep Disturbances: Rene E - CormierDokument6 SeitenSleep Disturbances: Rene E - CormierAdam GenturNoch keine Bewertungen
- Chapter 7 - States of ConsciousnessDokument7 SeitenChapter 7 - States of Consciousnessjeremypj100% (1)
- InsomniaDokument16 SeitenInsomniahappy tubeNoch keine Bewertungen
- Sleep DisordersDokument9 SeitenSleep DisordersCharmaine LowNoch keine Bewertungen
- Gen Psych - Lesson 5Dokument4 SeitenGen Psych - Lesson 5Ariadna ApolonioNoch keine Bewertungen
- Treatment of Primary InsomniaDokument8 SeitenTreatment of Primary Insomniadanny17phNoch keine Bewertungen
- Kousar Ishaq Khizra Khan Adeela Majeed Asia YasmeenDokument54 SeitenKousar Ishaq Khizra Khan Adeela Majeed Asia YasmeenKousar IshaqNoch keine Bewertungen
- Jcom Mar00 InsomniaDokument9 SeitenJcom Mar00 InsomniafarhantunichiaNoch keine Bewertungen
- Treatment of InsomniaDokument11 SeitenTreatment of Insomniajosif22Noch keine Bewertungen
- Narcolepsy: ClassificationDokument4 SeitenNarcolepsy: ClassificationCatalina MihaelaNoch keine Bewertungen
- OpenStax Psychology2e LN04Dokument7 SeitenOpenStax Psychology2e LN04Whitney CartwrightNoch keine Bewertungen
- ConsciousnessDokument10 SeitenConsciousnessShaira Mae CababaNoch keine Bewertungen
- Lecture 10Dokument24 SeitenLecture 10api-266895119Noch keine Bewertungen
- Sleep Paralysis and Sleep WalkingDokument23 SeitenSleep Paralysis and Sleep WalkingGunjan NautiyalNoch keine Bewertungen
- E Insomni9aDokument3 SeitenE Insomni9aAnni SholihahNoch keine Bewertungen
- Insomnia: non pharmacological approachVon EverandInsomnia: non pharmacological approachNoch keine Bewertungen
- Sleep - Biological RhythmsDokument5 SeitenSleep - Biological RhythmsAsad ullahNoch keine Bewertungen
- Sleep Wake DisordersDokument68 SeitenSleep Wake DisordersRashed ShatnawiNoch keine Bewertungen
- Patient Report NotesDokument15 SeitenPatient Report NotesRituparna GuptaNoch keine Bewertungen
- LPSY321Week088-5 2Dokument7 SeitenLPSY321Week088-5 2WilliamArugaNoch keine Bewertungen
- Insomnia 1Dokument17 SeitenInsomnia 1RizkaNoch keine Bewertungen
- Psy FinalDokument12 SeitenPsy FinalBegimaiNoch keine Bewertungen
- Cataplexy DissertationDokument12 SeitenCataplexy Dissertationgideon gideonNoch keine Bewertungen
- LAPMAN - 6130020049 Maulidatul Jinani FDokument22 SeitenLAPMAN - 6130020049 Maulidatul Jinani FFirda JinanNoch keine Bewertungen
- Modules 14 and 15 PsychDokument4 SeitenModules 14 and 15 PsychSarah AsifNoch keine Bewertungen
- Narcolepsy With CataplexyDokument13 SeitenNarcolepsy With CataplexySudeep SinghNoch keine Bewertungen
- Etiology and Treatment of Sleep Wake DisordersDokument8 SeitenEtiology and Treatment of Sleep Wake Disordersasma khalidNoch keine Bewertungen
- Disturbed Sleep PatternDokument4 SeitenDisturbed Sleep PatternTsaabitah AnwarNoch keine Bewertungen
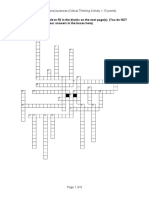
- Creative & Critical Thinking PaperDokument6 SeitenCreative & Critical Thinking PaperNazrul Naeem AsmawiNoch keine Bewertungen
- Sleep DisordersDokument41 SeitenSleep DisordersElRealManicheWemayNoch keine Bewertungen
- Rest and Sleep Study Guide AnswersDokument7 SeitenRest and Sleep Study Guide AnswersvickisscribdNoch keine Bewertungen
- Sleeping Disorders and Eating DisordersDokument54 SeitenSleeping Disorders and Eating DisordersHussain GauharNoch keine Bewertungen
- Topic08 ConsciousnessDokument18 SeitenTopic08 Consciousnessapi-19812879Noch keine Bewertungen
- Final Sleep 12Dokument27 SeitenFinal Sleep 12AndresPimentelAlvarezNoch keine Bewertungen
- Activity 51 NarcolepsyDokument6 SeitenActivity 51 NarcolepsyARAGON GEMMA LYNNoch keine Bewertungen
- P2 - Kelas 1Dokument46 SeitenP2 - Kelas 1meutiaputripuyNoch keine Bewertungen
- By: Reashnaa A/P Loganathan Yunisa Meutia Putri Zahra Fitrianti Preseptor: R.M. Haryadi Karyono, DR., SPKJDokument51 SeitenBy: Reashnaa A/P Loganathan Yunisa Meutia Putri Zahra Fitrianti Preseptor: R.M. Haryadi Karyono, DR., SPKJmeutiaputripuyNoch keine Bewertungen
- Referat Cerebral PalsyDokument17 SeitenReferat Cerebral PalsymeutiaputripuyNoch keine Bewertungen
- CTS CrsDokument38 SeitenCTS CrsmeutiaputripuyNoch keine Bewertungen
- By: Reashnaa A/P Loganathan Yunisa Meutia Putri Zahra Fitrianti Preseptor: R.M. Haryadi Karyono, DR., SPKJDokument51 SeitenBy: Reashnaa A/P Loganathan Yunisa Meutia Putri Zahra Fitrianti Preseptor: R.M. Haryadi Karyono, DR., SPKJmeutiaputripuyNoch keine Bewertungen
- CTS CrsDokument38 SeitenCTS CrsmeutiaputripuyNoch keine Bewertungen
- Causes of InsomniaDokument4 SeitenCauses of InsomniaSalmaPatimah OfficialNoch keine Bewertungen
- ZolpidemDokument2 SeitenZolpidemparthajiNoch keine Bewertungen
- Treatment of Psycho-Emotional With AcupunctureDokument5 SeitenTreatment of Psycho-Emotional With Acupuncturecharrie7Noch keine Bewertungen
- Can Amitriptyline Makes You Feel More Awake Instead of DrowsyDokument3 SeitenCan Amitriptyline Makes You Feel More Awake Instead of Drowsyteddypol100% (1)
- Final Project 3Dokument35 SeitenFinal Project 3api-666429985Noch keine Bewertungen
- Sleep and RestDokument85 SeitenSleep and RestJann ericka Jao100% (2)
- Supplementary 92 I. Choose The Word That Best Completes Each SentenceDokument4 SeitenSupplementary 92 I. Choose The Word That Best Completes Each Sentence19. Lê Khánh HuyềnNoch keine Bewertungen
- Sleep Disorders in DementiaDokument14 SeitenSleep Disorders in DementiadjnkmailNoch keine Bewertungen
- Harvard Doctor's Secrets For Better Sleep: HealthDokument17 SeitenHarvard Doctor's Secrets For Better Sleep: HealthContra_hourNoch keine Bewertungen
- Braverman Personality Type AssessmentDokument24 SeitenBraverman Personality Type AssessmentDaniela Stoica100% (2)
- Stress and Health - 2020 - Benham - Stress and Sleep in College Students Prior To and During The COVID 19 PandemicDokument12 SeitenStress and Health - 2020 - Benham - Stress and Sleep in College Students Prior To and During The COVID 19 PandemicchatarinaNoch keine Bewertungen
- Module e StreamlinedDokument7 SeitenModule e Streamlinedark1974Noch keine Bewertungen
- 1900 Parkyn Suggestive Therapeutics and HypnotismDokument443 Seiten1900 Parkyn Suggestive Therapeutics and HypnotismvictorNoch keine Bewertungen
- Biological Rhythms and SleepDokument50 SeitenBiological Rhythms and SleepChaz JosephsNoch keine Bewertungen
- Factors Affecting Sleep - MacaDokument15 SeitenFactors Affecting Sleep - Macamichan-fujiwara-2335Noch keine Bewertungen
- Ruqyah AdvertDokument1 SeiteRuqyah AdvertNana Aba DadzieNoch keine Bewertungen
- Utbk Bahasa Inggris 02Dokument2 SeitenUtbk Bahasa Inggris 02Riska Anggri MNoch keine Bewertungen
- Stilnox 10 MGDokument4 SeitenStilnox 10 MGperkinstop2000Noch keine Bewertungen
- Developing Instruments To Assess PersonalityDokument20 SeitenDeveloping Instruments To Assess Personalitygerielle mayoNoch keine Bewertungen
- P121.M3.Substance Related DisordersDokument33 SeitenP121.M3.Substance Related Disordersgwen awasNoch keine Bewertungen
- What Insomnia Can Do To Your Mind and BodyDokument2 SeitenWhat Insomnia Can Do To Your Mind and BodyMahmud AndreasNoch keine Bewertungen
- Foundations Study Guide FINAL EXAMDokument15 SeitenFoundations Study Guide FINAL EXAMigorot89100% (1)
- Krister Ann Jimenez ACTIVITY 14 ParagraphDokument17 SeitenKrister Ann Jimenez ACTIVITY 14 ParagraphKRISTER ANN JIMENEZNoch keine Bewertungen
- Barabasz, A, F., Olness, K., Boland, R and Kahn, S. (2010) Medical Hypnosis Primer: Clinical and Research EvidenceDokument3 SeitenBarabasz, A, F., Olness, K., Boland, R and Kahn, S. (2010) Medical Hypnosis Primer: Clinical and Research EvidenceEdwardGardnerNoch keine Bewertungen
- Argument Final DraftDokument5 SeitenArgument Final Draftapi-509051863Noch keine Bewertungen
- Sleep Medicine: Michael Gradisar, Greg Gardner, Hayley DohntDokument9 SeitenSleep Medicine: Michael Gradisar, Greg Gardner, Hayley DohntvipereejayNoch keine Bewertungen
- 25 Aug (Nitin Mishra Sir)Dokument51 Seiten25 Aug (Nitin Mishra Sir)AKASH CHIKTENoch keine Bewertungen