Das könnte Ihnen auch gefallen
- 1st Grade Sub PlansDokument89 Seiten1st Grade Sub PlansSouthern Brit100% (2)
- Aging with HIV: Psychological, Social, and Health IssuesVon EverandAging with HIV: Psychological, Social, and Health IssuesBewertung: 1 von 5 Sternen1/5 (1)
- Community Organizing Participatory Action ResearchDokument29 SeitenCommunity Organizing Participatory Action ResearchNoreen PadillaNoch keine Bewertungen
- The Effect of Parental Involvement On Student Performance.Dokument57 SeitenThe Effect of Parental Involvement On Student Performance.Anthony Okiria100% (3)
- Idealism in Education For Term PaperDokument6 SeitenIdealism in Education For Term PaperHaydee Requerme PelaezNoch keine Bewertungen
- Students' OrientationDokument123 SeitenStudents' OrientationJumar Gabrinao Gutang100% (1)
- Chapter 4 Profile of RespondentsDokument4 SeitenChapter 4 Profile of RespondentsJose BernelNoch keine Bewertungen
- Random Sampling DLPDokument7 SeitenRandom Sampling DLPjessica coronel100% (2)
- Obe MonitoringDokument2 SeitenObe MonitoringJeffer John100% (3)
- Teaching Is A Multifaceted ProfessionDokument4 SeitenTeaching Is A Multifaceted Professionamos ngonyamo88% (8)
- Hiv21 Ny d2 Flexner SlidesDokument52 SeitenHiv21 Ny d2 Flexner SlidesNimer Abdelhadi AliNoch keine Bewertungen
- Final Chapter 4Dokument11 SeitenFinal Chapter 4Quarl SanjuanNoch keine Bewertungen
- A Study On People'S Mental Health Conditions During COVID-19Dokument16 SeitenA Study On People'S Mental Health Conditions During COVID-19Ansu NitNoch keine Bewertungen
- Paper PPT Edited 20.4Dokument24 SeitenPaper PPT Edited 20.4shruti kumarNoch keine Bewertungen
- Rekomendasi Pemberian Covid-19Dokument35 SeitenRekomendasi Pemberian Covid-19ekaNoch keine Bewertungen
- Chapter 3 ResearchDokument3 SeitenChapter 3 ResearchNicole RheinNoch keine Bewertungen
- International Day of The Girl Child 2021Dokument12 SeitenInternational Day of The Girl Child 2021Yetunde OlagbujiNoch keine Bewertungen
- Afghanistan - Education Equity Profile For Adolescent GirlsDokument16 SeitenAfghanistan - Education Equity Profile For Adolescent GirlssalamNoch keine Bewertungen
- Position Paper To Commemorate The 2021 International Day of The Girl ChildDokument13 SeitenPosition Paper To Commemorate The 2021 International Day of The Girl ChildYetunde Olagbuji100% (1)
- Neuropsychology of An Addictive MindDokument45 SeitenNeuropsychology of An Addictive MindDr Nader KorhaniNoch keine Bewertungen
- EAP121 - WCW - First Draft Daoyuan LiDokument10 SeitenEAP121 - WCW - First Draft Daoyuan LiAlbert LiNoch keine Bewertungen
- Corrected Chapter 4 For Temptation WapwanyikaDokument22 SeitenCorrected Chapter 4 For Temptation WapwanyikaAshers NyawoNoch keine Bewertungen
- Data Analysis DoneDokument27 SeitenData Analysis DoneAnsu NitNoch keine Bewertungen
- The High/Scope Perry Preschool Study To Age 40: Larry Schweinhart & Jeanne MontieDokument13 SeitenThe High/Scope Perry Preschool Study To Age 40: Larry Schweinhart & Jeanne Montiejhoracios836318Noch keine Bewertungen
- Chapter 4 Profile of RespondentsDokument9 SeitenChapter 4 Profile of RespondentsJose BernelNoch keine Bewertungen
- CONFERENCEDokument12 SeitenCONFERENCETHONDYNALUNoch keine Bewertungen
- Encuesta de Electores Boricuas en Los Estados UnidosDokument23 SeitenEncuesta de Electores Boricuas en Los Estados UnidosEl Nuevo DíaNoch keine Bewertungen
- Presentation and Analysis of DataDokument9 SeitenPresentation and Analysis of DataMarge EscarchaNoch keine Bewertungen
- Hasil Analisis Survei Budaya PasienDokument47 SeitenHasil Analisis Survei Budaya Pasienanon_711785155Noch keine Bewertungen
- nextLI COVID-19 Long Island SurveyDokument60 SeitennextLI COVID-19 Long Island SurveyNewsdayNoch keine Bewertungen
- Health Education Future TrendsDokument29 SeitenHealth Education Future TrendsKathlyn PactorananNoch keine Bewertungen
- UntitledDokument23 SeitenUntitledKaryl CanaresNoch keine Bewertungen
- Module 7: Outpatient Management: Dengue ClinicalmanagementDokument22 SeitenModule 7: Outpatient Management: Dengue Clinicalmanagementjackie funtanillaNoch keine Bewertungen
- IZEA Insights - COVID19Dokument68 SeitenIZEA Insights - COVID19Melisa GutierrezNoch keine Bewertungen
- CQI HIM August 2021 PRHDokument16 SeitenCQI HIM August 2021 PRHAbdur Rashid KhanNoch keine Bewertungen
- The Perceptions of DKM 2C Students in PIS About SmokingDokument23 SeitenThe Perceptions of DKM 2C Students in PIS About SmokingAbdul Hakim RoslanNoch keine Bewertungen
- Pediatric Hiv - Zambia.Dokument59 SeitenPediatric Hiv - Zambia.Linus PuleNoch keine Bewertungen
- Connected Aging FrameworkDokument21 SeitenConnected Aging FrameworkRodrigo Flores EspinaNoch keine Bewertungen
- Colorectal Cancer Screening in Alberta ...Dokument23 SeitenColorectal Cancer Screening in Alberta ...cydolusNoch keine Bewertungen
- NAP (Harry P.) PDFDokument29 SeitenNAP (Harry P.) PDFaldyNoch keine Bewertungen
- AsdDokument11 SeitenAsdvui vuiNoch keine Bewertungen
- Farmers' Sustenance On Their Families' Basic NeedDokument27 SeitenFarmers' Sustenance On Their Families' Basic NeedRhobin Paul RespicioNoch keine Bewertungen
- Schools Daycares LatestDokument6 SeitenSchools Daycares LatestMindy WadleyNoch keine Bewertungen
- WWS PR 4 ViolenceDokument9 SeitenWWS PR 4 ViolenceGP ITNoch keine Bewertungen
- Description: Tags: Obj1-3Dokument7 SeitenDescription: Tags: Obj1-3anon-105538Noch keine Bewertungen
- Needs-Based HWF Planning Method - Scoping ReviewDokument24 SeitenNeeds-Based HWF Planning Method - Scoping ReviewJAMES AVOKA AsamaniNoch keine Bewertungen
- Effects of Social Media On Students' BehaviorDokument9 SeitenEffects of Social Media On Students' BehaviorMartinezNoch keine Bewertungen
- Access To Maternity Healthcare Service in Rural Bangladesh. A Study Area Sariakandi Upazila of Bogura DistrictDokument13 SeitenAccess To Maternity Healthcare Service in Rural Bangladesh. A Study Area Sariakandi Upazila of Bogura DistrictSajibNoch keine Bewertungen
- SIPDokument20 SeitenSIPSanket Bhondage0% (1)
- Final WB Poll Deck For Publishing 1 PDFDokument120 SeitenFinal WB Poll Deck For Publishing 1 PDFMira RadovicNoch keine Bewertungen
- Christine TableDokument2 SeitenChristine TableDINOPOL MARIELLENoch keine Bewertungen
- Method ResultDokument9 SeitenMethod Resultthiên ngân trầnNoch keine Bewertungen
- SPSS Baru JelasDokument12 SeitenSPSS Baru JelasMontaviana gale jamuraNoch keine Bewertungen
- What Clinicians Need To Know About Johnson & Johnson's Janssen COVID-19 VaccineDokument40 SeitenWhat Clinicians Need To Know About Johnson & Johnson's Janssen COVID-19 VaccineRamahari SihalNoch keine Bewertungen
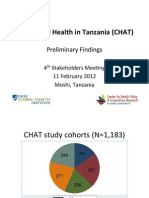
- Coping and Health in Tanzania (CHAT) : Preliminary FindingsDokument27 SeitenCoping and Health in Tanzania (CHAT) : Preliminary Findingskyle_hamilton9947Noch keine Bewertungen
- Source Political 2Dokument13 SeitenSource Political 2Jefferson NguyenNoch keine Bewertungen
- HIV in RwandaDokument29 SeitenHIV in RwandaRichard BalaisNoch keine Bewertungen
- Chapter 4: Analysis and InterpretationDokument26 SeitenChapter 4: Analysis and InterpretationHariNoch keine Bewertungen
- Image Based Abuse National Survey Summary Report 2017Dokument14 SeitenImage Based Abuse National Survey Summary Report 2017Kirsha Erika EstandarteNoch keine Bewertungen
- HPV Evaluation of Head and Neck Cancer Awareness and Screening Status in Jeddah, Saudi ArabiaDokument5 SeitenHPV Evaluation of Head and Neck Cancer Awareness and Screening Status in Jeddah, Saudi ArabiakarinagitakNoch keine Bewertungen
- AnalysisDokument4 SeitenAnalysissamy7541Noch keine Bewertungen
- Organic Food Consumption Among Vietnamese Shared by WorldLine TechnologyDokument39 SeitenOrganic Food Consumption Among Vietnamese Shared by WorldLine TechnologyDuy Nguyen Ho ThienNoch keine Bewertungen
- Blind SpotDokument76 SeitenBlind SpotDescriminalización.orgNoch keine Bewertungen
- 137-Article Text-512-1-10-20210127Dokument11 Seiten137-Article Text-512-1-10-2021012705Liana Febrianti SihotangNoch keine Bewertungen
- Kenya Consumer Survey ReportDokument60 SeitenKenya Consumer Survey Reportam6515094Noch keine Bewertungen
- Case Processing SummaryDokument4 SeitenCase Processing SummaryLuthfi LazuardiNoch keine Bewertungen
- Prakriti Analysis of COVID 19 Patients: An Observational StudyDokument12 SeitenPrakriti Analysis of COVID 19 Patients: An Observational StudySaurabh SumanNoch keine Bewertungen
- Discussions SamplesDokument45 SeitenDiscussions Sampleshayatullah hamdardNoch keine Bewertungen
- DTJ KA122-combinedDokument24 SeitenDTJ KA122-combinedIskola PanninéniNoch keine Bewertungen
- ATG MET 2 LESSON 2 EnthalpyDokument9 SeitenATG MET 2 LESSON 2 EnthalpyMarvin MoreteNoch keine Bewertungen
- Moon Phases Lesson 3Dokument3 SeitenMoon Phases Lesson 3api-489582725Noch keine Bewertungen
- Legal Latin TermsDokument100 SeitenLegal Latin TermsEdwino Nudo Barbosa Jr.Noch keine Bewertungen
- Geoscience Education An OverviewDokument38 SeitenGeoscience Education An OverviewjuanNoch keine Bewertungen
- Digital Literacy Training For Educators In-Service Training - Rosendale SewellDokument9 SeitenDigital Literacy Training For Educators In-Service Training - Rosendale Sewellapi-496471806Noch keine Bewertungen
- Health and Social Care Exemplar CourseworkDokument8 SeitenHealth and Social Care Exemplar Courseworkbcqy21t7100% (2)
- Miu Fs1 Worksheet Topic 7Dokument3 SeitenMiu Fs1 Worksheet Topic 7MIU MAE OBIDO MOSONESNoch keine Bewertungen
- ReflectionDokument1 SeiteReflectionFlora CoelieNoch keine Bewertungen
- Promoting Moral Education Among Senior High Students Through Co-Curricular Activities: Are There Challenges in Senior High Schools in Sunyani Municipality?Dokument8 SeitenPromoting Moral Education Among Senior High Students Through Co-Curricular Activities: Are There Challenges in Senior High Schools in Sunyani Municipality?Ijahss JournalNoch keine Bewertungen
- Differentiated L NewDokument60 SeitenDifferentiated L NewAbdul Nafiu YussifNoch keine Bewertungen
- DLL Week 5Dokument4 SeitenDLL Week 5Joyce Marace100% (1)
- Teachers Pedagogical Competence in School-Based Management: Case Study in A Public Secondary SchoolDokument7 SeitenTeachers Pedagogical Competence in School-Based Management: Case Study in A Public Secondary SchoolFitraAshariNoch keine Bewertungen
- Innovative Practice in Teacher EducationDokument4 SeitenInnovative Practice in Teacher EducationSourav PradhanNoch keine Bewertungen
- Gebhard Models of SupervisionDokument8 SeitenGebhard Models of SupervisionBritishCouncilAlgeriaNoch keine Bewertungen
- Sarah E. Ruff and Dr. Susan R. Boes, The University of West GeorgiaDokument10 SeitenSarah E. Ruff and Dr. Susan R. Boes, The University of West GeorgiaLaili Anisatu CMNoch keine Bewertungen
- Messenger As A Tool For Online LearningDokument29 SeitenMessenger As A Tool For Online LearningMary JoyNoch keine Bewertungen
- Mod 6Dokument4 SeitenMod 6farhanNoch keine Bewertungen
- 3is Q1 Module 3Dokument15 Seiten3is Q1 Module 3David King AvilaNoch keine Bewertungen
- HISTORY - 027 Class XI & XII (2022-23) Project WorkDokument5 SeitenHISTORY - 027 Class XI & XII (2022-23) Project WorkSnehaNoch keine Bewertungen
- Blooms Taxonomy Essay - Assignment 2Dokument6 SeitenBlooms Taxonomy Essay - Assignment 2api-493639541Noch keine Bewertungen
- Two Preceptorship Models PDFDokument6 SeitenTwo Preceptorship Models PDFNur Shafridah Mr-GenNoch keine Bewertungen