Das könnte Ihnen auch gefallen
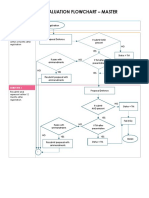
- Master by Research-FTMK Evaluation FlowchartDokument2 SeitenMaster by Research-FTMK Evaluation FlowchartFitrah RumaisaNoch keine Bewertungen
- Canopus BerylGreenDokument62 SeitenCanopus BerylGreenDamjacht QahwaNoch keine Bewertungen
- 525 Sample Scholarship Recommendation Letter Current or Former StudentDokument1 Seite525 Sample Scholarship Recommendation Letter Current or Former StudentKoran RakyatNoch keine Bewertungen
- What Is A Survey PaperDokument16 SeitenWhat Is A Survey PaperFitrah RumaisaNoch keine Bewertungen
- IEEE Paper FormatDokument3 SeitenIEEE Paper FormatSanhith RaoNoch keine Bewertungen
- Vega NoAnimationDokument86 SeitenVega NoAnimationAthikaymNoch keine Bewertungen
- Rapid Miner 4.4 TutorialDokument677 SeitenRapid Miner 4.4 Tutorialejrobb81Noch keine Bewertungen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (120)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Journal of Medicinal Plants Research VolDokument19 SeitenJournal of Medicinal Plants Research VolAtheena Jin Anjelle SeveroNoch keine Bewertungen
- General DeclarationDokument1 SeiteGeneral DeclarationPos SMB IINoch keine Bewertungen
- Dry Eye Disease After Refractive SurgeryDokument6 SeitenDry Eye Disease After Refractive SurgeryCastiglianoNoch keine Bewertungen
- Hoarseness-Causes and TreatmentsDokument33 SeitenHoarseness-Causes and TreatmentsSatrio WisnugrohoNoch keine Bewertungen
- Chart Medical Eligibility Contraceptives EnglishDokument1 SeiteChart Medical Eligibility Contraceptives EnglishTiang Soon TeckNoch keine Bewertungen
- T2DM PracticalGuide 20190718 FA Ebook2Dokument80 SeitenT2DM PracticalGuide 20190718 FA Ebook2Nokoline HuNoch keine Bewertungen
- Hematology Unit: Complete Blood Count (CBC)Dokument2 SeitenHematology Unit: Complete Blood Count (CBC)Rasha ElbannaNoch keine Bewertungen
- Viral Diseases - Mechanisms of Microbial InfectionsDokument105 SeitenViral Diseases - Mechanisms of Microbial InfectionspolypeptideNoch keine Bewertungen
- Chamani Essay VAPEDokument2 SeitenChamani Essay VAPEChamani MadawalaNoch keine Bewertungen
- Letting Go by Atul GawandeDokument18 SeitenLetting Go by Atul Gawandetakoyakilovers100% (2)
- Maternal and Child HealthDokument60 SeitenMaternal and Child HealthStar AcademyNoch keine Bewertungen
- Module Answers 1 60 MCN 2Dokument151 SeitenModule Answers 1 60 MCN 2bekbekk cabahug100% (6)
- FibromaDokument3 SeitenFibromaAsiyath HNoch keine Bewertungen
- Canine Influenza FactsDokument5 SeitenCanine Influenza FactsWIS Digital News StaffNoch keine Bewertungen
- Konsep Wound ManajemenDokument24 SeitenKonsep Wound ManajemenNiken DewiNoch keine Bewertungen
- Intership Questionnaire For Cleaning Tools Used in HospitalsDokument4 SeitenIntership Questionnaire For Cleaning Tools Used in HospitalsSomannaNoch keine Bewertungen
- Checklist - Assisting - Circulating DeliveryDokument2 SeitenChecklist - Assisting - Circulating DeliveryLue Vigiem M. GuiasNoch keine Bewertungen
- 2) Megaloblastic AnemiaDokument17 Seiten2) Megaloblastic AnemiaAndrea Aprilia100% (1)
- 32 Oet Reading Summary 2.0-697-717Dokument21 Seiten32 Oet Reading Summary 2.0-697-717Santhus100% (7)
- J Clin Aph - Guidelines TADokument95 SeitenJ Clin Aph - Guidelines TAadainuri100% (1)
- CLICO Group Health and Life Coverage 1Dokument12 SeitenCLICO Group Health and Life Coverage 1buckianNoch keine Bewertungen
- Complication of Sinus DiseaseDokument27 SeitenComplication of Sinus DiseaseukhuholicNoch keine Bewertungen
- Psychotropic Drug Overdose The Death of The Hollywood Celebrity Heath LedgerDokument5 SeitenPsychotropic Drug Overdose The Death of The Hollywood Celebrity Heath LedgerlalipredebonNoch keine Bewertungen
- EMS Airflow BrochureDokument2 SeitenEMS Airflow BrochureMELHEM_J8008Noch keine Bewertungen
- NCP - Gestational DiabetesDokument2 SeitenNCP - Gestational DiabetesKailah Rose CabantoyNoch keine Bewertungen
- Acute Complications of Diabetes Mellitus: Hypoglycemia and Hypoglycemic ComaDokument30 SeitenAcute Complications of Diabetes Mellitus: Hypoglycemia and Hypoglycemic ComaCristinaGheorgheNoch keine Bewertungen
- Intramedullary Spinal Cord Tumors: Part II - Management Options and OutcomesDokument10 SeitenIntramedullary Spinal Cord Tumors: Part II - Management Options and OutcomeszixzaxoffNoch keine Bewertungen
- List of Diseases and Ailments With UrduDokument7 SeitenList of Diseases and Ailments With Urduaik hindustaniNoch keine Bewertungen
- Dade InnovinDokument7 SeitenDade InnovinchaiNoch keine Bewertungen
- Cryptosporidiosis in Ruminants: Update and Current Therapeutic ApproachesDokument8 SeitenCryptosporidiosis in Ruminants: Update and Current Therapeutic ApproachesDrivailaNoch keine Bewertungen