Das könnte Ihnen auch gefallen
- From Evidence to Clinical Practice in Diabetes ManagementDokument40 SeitenFrom Evidence to Clinical Practice in Diabetes ManagementscribdNoch keine Bewertungen
- Metabolic Syndrome, Diabetes, and Cardiovascular Disease: Implications for Preventive CardiologyDokument36 SeitenMetabolic Syndrome, Diabetes, and Cardiovascular Disease: Implications for Preventive CardiologyAlvianridersNoch keine Bewertungen
- Cardiovascular Risk in Chronic Renal DiseaseDokument36 SeitenCardiovascular Risk in Chronic Renal DiseaseahkyenNoch keine Bewertungen
- Treatment Based On: Pathophysiology of HyperglycemiaDokument38 SeitenTreatment Based On: Pathophysiology of HyperglycemiaRoby KieranNoch keine Bewertungen
- DM and NeurologyDokument43 SeitenDM and NeurologySurat TanprawateNoch keine Bewertungen
- CVD in Diabetes - EADSG 2016Dokument57 SeitenCVD in Diabetes - EADSG 2016OmarNoch keine Bewertungen
- Atorvastatin Statin in CVD ManagementDokument37 SeitenAtorvastatin Statin in CVD ManagementSriNoch keine Bewertungen
- Statins in CVD Management: Is Just Lipid Lowering Enough?Dokument37 SeitenStatins in CVD Management: Is Just Lipid Lowering Enough?SriNoch keine Bewertungen
- Management of T2DMDokument54 SeitenManagement of T2DMdesyNoch keine Bewertungen
- Dangas 2014 DiabetesDokument9 SeitenDangas 2014 Diabetesmoroni.cayseNoch keine Bewertungen
- Austin AndrologyDokument4 SeitenAustin AndrologyAustin Publishing GroupNoch keine Bewertungen
- Management of Hyperglycemia and Diabetes in The HospitalDokument46 SeitenManagement of Hyperglycemia and Diabetes in The HospitalvinoadhiyogaNoch keine Bewertungen
- Evidence Based MedicineDokument22 SeitenEvidence Based MedicineLastry WardaniNoch keine Bewertungen
- Cystatin C - Conferences and PublicationsDokument9 SeitenCystatin C - Conferences and PublicationsMedo MedoNoch keine Bewertungen
- Blood Pressure Management in Patients With DiabetesDokument8 SeitenBlood Pressure Management in Patients With DiabetesHoài ThươngNoch keine Bewertungen
- How To Position Finerenone in The Treatment Algorithm For Type 2 Diabetes With Renal Complication - GPMPDokument27 SeitenHow To Position Finerenone in The Treatment Algorithm For Type 2 Diabetes With Renal Complication - GPMPTaufiqurrokhman RofiiNoch keine Bewertungen
- Edit Virtual HR Managing Dyslipidemia in Special PopulationDokument38 SeitenEdit Virtual HR Managing Dyslipidemia in Special PopulationIkmah FauzanNoch keine Bewertungen
- Diabetes Update: Facts Show Growing Prevalence and Costs Despite Intensifying TreatmentDokument28 SeitenDiabetes Update: Facts Show Growing Prevalence and Costs Despite Intensifying TreatmentPilar Victoria Arrieta VegaNoch keine Bewertungen
- Dyslipidemia Management in Diabetic PatientsDokument31 SeitenDyslipidemia Management in Diabetic PatientsaprinaaaNoch keine Bewertungen
- Strengthening The Global Risk ManagementDokument31 SeitenStrengthening The Global Risk ManagementSriNoviantiNoch keine Bewertungen
- Role of Finerenone As New Pillar in CKD Management in T2D Patients - GPMPDokument29 SeitenRole of Finerenone As New Pillar in CKD Management in T2D Patients - GPMPTaufiqurrokhman RofiiNoch keine Bewertungen
- Update On Renal Disease For The Dental PractitionerDokument8 SeitenUpdate On Renal Disease For The Dental PractitionerJuan Pablo VargasNoch keine Bewertungen
- Articol Rev Med Chirrefacut OvidiuDokument8 SeitenArticol Rev Med Chirrefacut OvidiuNicu IacobNoch keine Bewertungen
- Anemia: Chronic Kidney DiseaseDokument12 SeitenAnemia: Chronic Kidney DiseasetyasNoch keine Bewertungen
- Association of Diabetes Mellitus and Its Types With In-HospitalDokument7 SeitenAssociation of Diabetes Mellitus and Its Types With In-HospitalJunior CasanaNoch keine Bewertungen
- Diabetic NephropathyDokument38 SeitenDiabetic NephropathySwapnaNoch keine Bewertungen
- Diabetul Zaharat Tip2 O Chemare La ActiuneDokument23 SeitenDiabetul Zaharat Tip2 O Chemare La ActiuneGabriela ManolescuNoch keine Bewertungen
- DIABertelt2017 14Dokument7 SeitenDIABertelt2017 14marsim92Noch keine Bewertungen
- Slide RTD Traditionalist BaruDokument48 SeitenSlide RTD Traditionalist BaruGanjar AdityoNoch keine Bewertungen
- Unmeet Need Is LDL-C Lowering When Regular Statin Wont DoDokument40 SeitenUnmeet Need Is LDL-C Lowering When Regular Statin Wont Doyan salvianto100% (1)
- Dyslipidaemias 2019Dokument30 SeitenDyslipidaemias 2019Adinda DianNoch keine Bewertungen
- Association of Blood Pressure Control and Metabolic Syndrome With Cardiovascular Risk in Elderly Japanese: JATOS StudyDokument7 SeitenAssociation of Blood Pressure Control and Metabolic Syndrome With Cardiovascular Risk in Elderly Japanese: JATOS StudyRobertoNoch keine Bewertungen
- Global Risk of Cardiovascular Disease: Assessment and ApplicationDokument18 SeitenGlobal Risk of Cardiovascular Disease: Assessment and ApplicationEmdan SengadjiNoch keine Bewertungen
- 2016 Article 69Dokument10 Seiten2016 Article 69Rhowy Al-mu'izzahNoch keine Bewertungen
- ADVANCE-On EASD Study Rationale and DesignDokument26 SeitenADVANCE-On EASD Study Rationale and Designmariatul fithriasariNoch keine Bewertungen
- Prof Kiking Ritarwan - STROKE-KRTDokument64 SeitenProf Kiking Ritarwan - STROKE-KRTBernard Fernandes PanjaitanNoch keine Bewertungen
- ProjectEcho August9 Didactic ArakakiDokument26 SeitenProjectEcho August9 Didactic ArakakiNakamura AsukaNoch keine Bewertungen
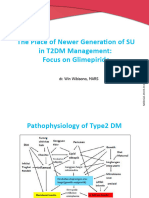
- 2018 RTD Slide - The Place of Newer Generation SUDokument30 Seiten2018 RTD Slide - The Place of Newer Generation SUAlka AlkaNoch keine Bewertungen
- Residual Risk: What Risk Remains After LDL-C Management and Intensive Therapy?Dokument7 SeitenResidual Risk: What Risk Remains After LDL-C Management and Intensive Therapy?krispongNoch keine Bewertungen
- Gagal Ginjal (2) : Institute of Health Sciences BanyuwangiDokument54 SeitenGagal Ginjal (2) : Institute of Health Sciences BanyuwangiAdek Prayugi PutriNoch keine Bewertungen
- Empagliflozin in Prevention of Cardiovascular Disease Among Patients With Diabetes Mellitus Type 2Dokument4 SeitenEmpagliflozin in Prevention of Cardiovascular Disease Among Patients With Diabetes Mellitus Type 2tb9Noch keine Bewertungen
- Cinical Inertia - Final Release PDFDokument43 SeitenCinical Inertia - Final Release PDFrent3010Noch keine Bewertungen
- Diabetes For Cardiologists Practical Issues in Diagnosis and ManagementDokument12 SeitenDiabetes For Cardiologists Practical Issues in Diagnosis and ManagementLuis Alberto OrtizNoch keine Bewertungen
- Study of Anaemia in Type 2 Diabetes Mellitus, Risk Factor For The Presence and Severity of Micro Vascular Complication, Diabetic RetinopathyDokument7 SeitenStudy of Anaemia in Type 2 Diabetes Mellitus, Risk Factor For The Presence and Severity of Micro Vascular Complication, Diabetic RetinopathyIJAR JOURNALNoch keine Bewertungen
- Lipid Treatments in Cardiologic, Metabolic and Diabetics: From Guideline To Clinical PracticeDokument65 SeitenLipid Treatments in Cardiologic, Metabolic and Diabetics: From Guideline To Clinical PracticeRoby KieranNoch keine Bewertungen
- b9fb7635770701193491250 PACE ACROSS T2D Module B 11aug2015 000419Dokument38 Seitenb9fb7635770701193491250 PACE ACROSS T2D Module B 11aug2015 000419Mia DangaNoch keine Bewertungen
- X. Tillin 2011 DT2Dokument6 SeitenX. Tillin 2011 DT2Juan Carlos FloresNoch keine Bewertungen
- Pemberian Insulin KMBDokument36 SeitenPemberian Insulin KMBerdhian jatiNoch keine Bewertungen
- 2019 Article 612Dokument17 Seiten2019 Article 612Asad NawazNoch keine Bewertungen
- Strategies-S3-Hyperglycemic-Emergencies 1Dokument82 SeitenStrategies-S3-Hyperglycemic-Emergencies 1Wai Kwong ChiuNoch keine Bewertungen
- Cardiovascular Outcome Trials: A History and Look to the FutureDokument9 SeitenCardiovascular Outcome Trials: A History and Look to the Futuresony chawlaNoch keine Bewertungen
- Cerebrovascular Diseases: Global Burden and Prevention StrategiesDokument28 SeitenCerebrovascular Diseases: Global Burden and Prevention StrategiesbagussofianNoch keine Bewertungen
- Effects DMCEA01Dokument11 SeitenEffects DMCEA01milmrch523Noch keine Bewertungen
- Correlation Between Systemic Risk Factors and Diabetic Macular Edema in Diabetes Mellitus - Dian Paramitasari 1Dokument8 SeitenCorrelation Between Systemic Risk Factors and Diabetic Macular Edema in Diabetes Mellitus - Dian Paramitasari 1Hutami Sri UmmiyatiNoch keine Bewertungen
- Interpretation of Cardiovascular Outcome TrialsDokument9 SeitenInterpretation of Cardiovascular Outcome TrialsmagreaNoch keine Bewertungen
- Prevalence of Conventional Risk Factors and Lipid Profiles in Patients With Acute Coronary Syndrome and Significant Coronary DiseaseDokument19 SeitenPrevalence of Conventional Risk Factors and Lipid Profiles in Patients With Acute Coronary Syndrome and Significant Coronary DiseaseUyên LêNoch keine Bewertungen
- Preventing Cardiovascular Disease in Patients With.2 PDFDokument3 SeitenPreventing Cardiovascular Disease in Patients With.2 PDFbacharelado2010Noch keine Bewertungen
- Management of T Dmintheeraof Cardiovascular Outcome TrialDokument43 SeitenManagement of T Dmintheeraof Cardiovascular Outcome TrialHeri Agung SetiawanNoch keine Bewertungen
- Management of Dyslipidemia in Adults With DiabetesDokument19 SeitenManagement of Dyslipidemia in Adults With DiabetesWahyuningsih HamidNoch keine Bewertungen
- Managing Cardiovascular Complications in DiabetesVon EverandManaging Cardiovascular Complications in DiabetesNoch keine Bewertungen
- Tabel ICD 10 English Indonesia LengkapDokument432 SeitenTabel ICD 10 English Indonesia LengkaptwindaNoch keine Bewertungen
- TB and Lung CancerDokument26 SeitenTB and Lung CanceraprinaaaNoch keine Bewertungen
- Dyslipidemia Management in Diabetic PatientsDokument31 SeitenDyslipidemia Management in Diabetic PatientsaprinaaaNoch keine Bewertungen
- Bpjs Insulin 2015Dokument34 SeitenBpjs Insulin 2015aprinaaaNoch keine Bewertungen
- Breast Cancer - ETDokument21 SeitenBreast Cancer - ETaprinaaaNoch keine Bewertungen
- 4.release How To Intensify Basal Insulin With Premix and Basal Bolus ApproachDokument42 Seiten4.release How To Intensify Basal Insulin With Premix and Basal Bolus ApproachaprinaaaNoch keine Bewertungen
- Tabel ICD 10 English Indonesia LengkapDokument432 SeitenTabel ICD 10 English Indonesia LengkaptwindaNoch keine Bewertungen
- Hypertension. Pengendalian Faktor Risiko Penyakit Kardiovaskular DINKES TK 1 BJM 23 Maret 2016Dokument38 SeitenHypertension. Pengendalian Faktor Risiko Penyakit Kardiovaskular DINKES TK 1 BJM 23 Maret 2016aprinaaaNoch keine Bewertungen
- Recurrent PancreatitisDokument9 SeitenRecurrent PancreatitisAv RienNoch keine Bewertungen
- Necrotizing PancreatitisDokument2 SeitenNecrotizing PancreatitisAv RienNoch keine Bewertungen
- Tatalaksana Dan Titrasi InsulinDokument34 SeitenTatalaksana Dan Titrasi InsulinaprinaaaNoch keine Bewertungen
- Recurrent PancreatitisDokument9 SeitenRecurrent PancreatitisAv RienNoch keine Bewertungen
- Non Biliary PancreatitisDokument9 SeitenNon Biliary PancreatitisaprinaaaNoch keine Bewertungen
- Non Biliary PancreatitisDokument9 SeitenNon Biliary PancreatitisaprinaaaNoch keine Bewertungen
- Fever and Abd - PainDokument9 SeitenFever and Abd - PainAv RienNoch keine Bewertungen
- Functional Dyspepsia: Recent Advances in Pathophysiology: Update ArticleDokument5 SeitenFunctional Dyspepsia: Recent Advances in Pathophysiology: Update ArticleDen BollongNoch keine Bewertungen
- How Brain Science Can Inform Architectural DesignDokument12 SeitenHow Brain Science Can Inform Architectural DesignadrianmoleavinNoch keine Bewertungen
- Siddha Therapeutic Index - 18-Article Text-133-1-10-20210308Dokument7 SeitenSiddha Therapeutic Index - 18-Article Text-133-1-10-20210308Dr.kali.vijay kumkarNoch keine Bewertungen
- VMC Customer Service Complaint and Letter of DemandDokument3 SeitenVMC Customer Service Complaint and Letter of DemandJames Alan BushNoch keine Bewertungen
- A Comparison of Muscle Strength and Flexibility Between The Preferred and Non Preferred Leg in English Soccer PlayersDokument10 SeitenA Comparison of Muscle Strength and Flexibility Between The Preferred and Non Preferred Leg in English Soccer PlayersMalikiNoch keine Bewertungen
- World03 30 16Dokument40 SeitenWorld03 30 16The WorldNoch keine Bewertungen
- Check Your English Vocabulary For MedicineDokument59 SeitenCheck Your English Vocabulary For MedicineCentru RefillNoch keine Bewertungen
- Neonatal Developemental MilestonesDokument4 SeitenNeonatal Developemental MilestonesSubha DeepNoch keine Bewertungen
- Maharashtra Government PGM Admissions 2015-2016 Round 2 Selection ListDokument30 SeitenMaharashtra Government PGM Admissions 2015-2016 Round 2 Selection ListAbhinav BhardwajNoch keine Bewertungen
- Medicine, Coptic.: Chronological Table of Ostraca and Papyri Dealing With MedicineDokument7 SeitenMedicine, Coptic.: Chronological Table of Ostraca and Papyri Dealing With MedicinePaula VeigaNoch keine Bewertungen
- Pes WesDokument12 SeitenPes WesjotapintorNoch keine Bewertungen
- Work Sheet, Lesson 5Dokument7 SeitenWork Sheet, Lesson 5WasimHassanShahNoch keine Bewertungen
- WeeFIM Score Sheet (MS Word)Dokument4 SeitenWeeFIM Score Sheet (MS Word)Siti Maryam Rosyidah0% (2)
- IMCI Chart BookletDokument66 SeitenIMCI Chart Bookletnorwin_033875Noch keine Bewertungen
- Top 5 Strength Exercises For RugbyDokument4 SeitenTop 5 Strength Exercises For RugbyPaul Tinashe KatuliibaNoch keine Bewertungen
- Digital Paper Trail DPTDokument5 SeitenDigital Paper Trail DPTapi-549372008Noch keine Bewertungen
- Antioxidant and Antimicrobial Activities of Pink Guava Leaves and SeedsDokument10 SeitenAntioxidant and Antimicrobial Activities of Pink Guava Leaves and SeedsRobbyNoch keine Bewertungen
- Ancient MedicineDokument3 SeitenAncient MedicineJasonNoch keine Bewertungen
- Pharmacology For Nurses by Diane Pacitti Blaine T. SmithDokument570 SeitenPharmacology For Nurses by Diane Pacitti Blaine T. SmithJessica Anis0% (1)
- Task Oriented Circuit Training Improves Ambulatory Functions in Acute Stroke A Randomized Controlled TrialDokument7 SeitenTask Oriented Circuit Training Improves Ambulatory Functions in Acute Stroke A Randomized Controlled TrialadlestariNoch keine Bewertungen
- Chapter - 3 Medical Negligence and It'S Relation With Consumer Protection Act, 1986Dokument67 SeitenChapter - 3 Medical Negligence and It'S Relation With Consumer Protection Act, 1986Soumiki GhoshNoch keine Bewertungen
- Hospital List 06052016Dokument5 SeitenHospital List 06052016Azhar ThireiNoch keine Bewertungen
- Clinical Reasoning FCPDokument39 SeitenClinical Reasoning FCPUlan NoputriNoch keine Bewertungen
- 2322 Part B DCHB IndoreDokument278 Seiten2322 Part B DCHB Indoreksanjay209Noch keine Bewertungen
- Guidance For Installation and Testing AcceptanceDokument32 SeitenGuidance For Installation and Testing AcceptanceMun WaiNoch keine Bewertungen
- UrinalysisDokument16 SeitenUrinalysisJestha Parayno De Vera100% (6)
- Health and its failure: Causes, Types, and Prevention of DiseasesDokument9 SeitenHealth and its failure: Causes, Types, and Prevention of DiseasesAbhimanyu BahreeNoch keine Bewertungen
- Risk of Ovarian Cancer Algorithm (ROCA) Using Serial CA 125Dokument9 SeitenRisk of Ovarian Cancer Algorithm (ROCA) Using Serial CA 125primadian atnaryanNoch keine Bewertungen
- Breast, EndocrineDokument247 SeitenBreast, EndocrineRajan VaithianathanNoch keine Bewertungen
- Acute Myocardial InfarctionDokument35 SeitenAcute Myocardial Infarctionvirnzrobz80% (10)