Das könnte Ihnen auch gefallen
- Kasus Maternal CovidDokument21 SeitenKasus Maternal CovidLanny Margaretha BarutuNoch keine Bewertungen
- Edema Paru Pit FM SMGDokument36 SeitenEdema Paru Pit FM SMGAnonymous ZrLxxRUr9zNoch keine Bewertungen
- LAPHAR NEFRO 1 November 2022Dokument5 SeitenLAPHAR NEFRO 1 November 2022dryubyNoch keine Bewertungen
- Syok Hipovolemic Ec. Dengue Infection Najip WidiDokument15 SeitenSyok Hipovolemic Ec. Dengue Infection Najip WidiwidiNoch keine Bewertungen
- PSGNPPTDokument70 SeitenPSGNPPTJirran CabatinganNoch keine Bewertungen
- Case DR SugoroDokument22 SeitenCase DR SugorowilliamNoch keine Bewertungen
- Lapkas IGD - TDPDokument35 SeitenLapkas IGD - TDPPutri Widiya PusvitaNoch keine Bewertungen
- Morning Report: Physician in ChargeDokument11 SeitenMorning Report: Physician in ChargeImam Mi'raj SuprayogaNoch keine Bewertungen
- Yosefin Eka Pembimbing: Dr. Anik W., Sp. PK (K)Dokument33 SeitenYosefin Eka Pembimbing: Dr. Anik W., Sp. PK (K)Yosefin EkaNoch keine Bewertungen
- DK IKA 1 - Ogie RevDokument193 SeitenDK IKA 1 - Ogie RevhariogieNoch keine Bewertungen
- Mappimg Kamar 1 Dan 5Dokument4 SeitenMappimg Kamar 1 Dan 5Satrya DitaNoch keine Bewertungen
- 22-11-22 RicuDokument316 Seiten22-11-22 RicuJhon WickNoch keine Bewertungen
- MR R 26 6-3 2017 MR W Fix AMS Septic AKIDokument15 SeitenMR R 26 6-3 2017 MR W Fix AMS Septic AKISafira RNoch keine Bewertungen
- Pengawasan 16.10.22Dokument7 SeitenPengawasan 16.10.22Ilmiah Program studi ObginNoch keine Bewertungen
- 22-11-22 RicuDokument303 Seiten22-11-22 RicuJhon WickNoch keine Bewertungen
- Morning Report Thursday, April 12st 2018: Mad/Rhs/IssDokument16 SeitenMorning Report Thursday, April 12st 2018: Mad/Rhs/IssIrene Sri Malem SembiringNoch keine Bewertungen
- BORANGDokument33 SeitenBORANGDewi WangsaNoch keine Bewertungen
- Case ComplexDokument32 SeitenCase ComplexMuhammad ApriyandaNoch keine Bewertungen
- LAPHAR NEFRO 4 November 2022Dokument6 SeitenLAPHAR NEFRO 4 November 2022dryubyNoch keine Bewertungen
- Bab IDokument76 SeitenBab INubhy NubhyNoch keine Bewertungen
- Responsi Stemi Dr. Tuko SP - JP FixDokument56 SeitenResponsi Stemi Dr. Tuko SP - JP FixcintaNoch keine Bewertungen
- Summary of Data Base: MR Z/41 YO/W.26Dokument35 SeitenSummary of Data Base: MR Z/41 YO/W.26Faricha KurniaNoch keine Bewertungen
- Asalamualaikum Kakak AyukDokument4 SeitenAsalamualaikum Kakak AyukIlmiah Program studi ObginNoch keine Bewertungen
- Morning Report CKDDokument20 SeitenMorning Report CKDjoe joeNoch keine Bewertungen
- Parade Bedah Vaskular: Sabtu, 17 Juli 2021Dokument40 SeitenParade Bedah Vaskular: Sabtu, 17 Juli 2021DICKY PANDUWINATANoch keine Bewertungen
- Laporan Kasus DSS: Oleh Dr. Betharia Susi Simamora Dibimbing Oleh Dr. NOVALIN SUMENDAP, Sp.ADokument41 SeitenLaporan Kasus DSS: Oleh Dr. Betharia Susi Simamora Dibimbing Oleh Dr. NOVALIN SUMENDAP, Sp.Achristiealexa13100% (1)
- Case 1 ChindiDokument30 SeitenCase 1 ChindiRachindi Qory TrysiaNoch keine Bewertungen
- Pressus IPDDokument24 SeitenPressus IPDAdistha TofanoNoch keine Bewertungen
- Carmiasih 49 Diabetic FootDokument21 SeitenCarmiasih 49 Diabetic Footdevi_pramulawatiNoch keine Bewertungen
- Unusual Complication in DKA: Dr. Swapna Fellow in Paediatric Intensive Care Ich&Hc Guide: Dr. PoovazhagiDokument20 SeitenUnusual Complication in DKA: Dr. Swapna Fellow in Paediatric Intensive Care Ich&Hc Guide: Dr. Poovazhagikannan73drNoch keine Bewertungen
- STEMIDokument33 SeitenSTEMIfauziahNoch keine Bewertungen
- Death CaseDokument21 SeitenDeath Casesavina hasbianiNoch keine Bewertungen
- Death Case CKDDokument40 SeitenDeath Case CKDIpong DipongNoch keine Bewertungen
- COVID 27 Februari 2021 PagiDokument109 SeitenCOVID 27 Februari 2021 PagiRifda NabilaNoch keine Bewertungen
- Morning Report Wednesday, April 30 2015: Coass in Charge Wahyu F Supervisor: Dr. Putu Moda A, SP - PDDokument8 SeitenMorning Report Wednesday, April 30 2015: Coass in Charge Wahyu F Supervisor: Dr. Putu Moda A, SP - PDYulia ManaweanNoch keine Bewertungen
- Duty Ricky CKD R.28 NewDokument4 SeitenDuty Ricky CKD R.28 NewRicky Cornelius TariganNoch keine Bewertungen
- JusniDokument14 SeitenJusniSarahNoch keine Bewertungen
- CASE PRES PreeclampsiaDokument51 SeitenCASE PRES PreeclampsiaRaiza Love Caparas-PablicoNoch keine Bewertungen
- CBD Iccu 2Dokument29 SeitenCBD Iccu 2Jumadi SyhuraNoch keine Bewertungen
- Disjag Baru CKDDokument17 SeitenDisjag Baru CKDNorma Juwita MNoch keine Bewertungen
- Sekar KSP - Hypoglicemia Ec Tipe 2 DMDokument28 SeitenSekar KSP - Hypoglicemia Ec Tipe 2 DMdianarahimmNoch keine Bewertungen
- Pembimbing: Dr. Adi Purnawarman, SP - JP: Morning ReportDokument25 SeitenPembimbing: Dr. Adi Purnawarman, SP - JP: Morning ReportListiani AyuNoch keine Bewertungen
- MR Sindrom Nefrotik 1 Agustus 17Dokument12 SeitenMR Sindrom Nefrotik 1 Agustus 17Ridho CahyaNoch keine Bewertungen
- DK Endokrin 1 - Thyroid StormDokument37 SeitenDK Endokrin 1 - Thyroid StormlaurachristianiNoch keine Bewertungen
- Morning Report: Dr. Dikara WS Maulidy, SP - PDDokument24 SeitenMorning Report: Dr. Dikara WS Maulidy, SP - PDBethari Abi SafitriNoch keine Bewertungen
- Pebimbing: Dr. Sylviasari RisgiantiniDokument17 SeitenPebimbing: Dr. Sylviasari RisgiantiniDona ViolitaNoch keine Bewertungen
- Pubic Bone Stable - Closed FractureDokument31 SeitenPubic Bone Stable - Closed FractureFelicia SaraswatiNoch keine Bewertungen
- Approach To ThrombophiliaDokument58 SeitenApproach To ThrombophiliaVanessa EdizaNoch keine Bewertungen
- POMR Satiti Acute CholangitisDokument30 SeitenPOMR Satiti Acute CholangitisIka AyuNoch keine Bewertungen
- Duty Report: August 9th, 2021Dokument13 SeitenDuty Report: August 9th, 2021LyDia Sarah ShabrinaNoch keine Bewertungen
- Slide - Muh Rakib Yunus - Unstable Angina PectorisDokument30 SeitenSlide - Muh Rakib Yunus - Unstable Angina PectorisbarujuannaNoch keine Bewertungen
- Lapsus CHFDokument28 SeitenLapsus CHFMutmainnah InnahNoch keine Bewertungen
- Systemic Lupus ErythematosusDokument89 SeitenSystemic Lupus ErythematosusIke RilleraNoch keine Bewertungen
- Parade Bedah Vaskular: Sabtu, 17 Juli 2021Dokument43 SeitenParade Bedah Vaskular: Sabtu, 17 Juli 2021DICKY PANDUWINATANoch keine Bewertungen
- Morning ReportDokument17 SeitenMorning Reportjoe joeNoch keine Bewertungen
- Morning Report Rsud Provinsi Papua Barat: Rabu, 9 Maret 2022Dokument59 SeitenMorning Report Rsud Provinsi Papua Barat: Rabu, 9 Maret 2022Khoirunnisa PuaradaNoch keine Bewertungen
- Pasien Raber Per TGL 10 November 2023 FKDokument5 SeitenPasien Raber Per TGL 10 November 2023 FKmasitha yusmarNoch keine Bewertungen
- Morning Report 11 JuliDokument19 SeitenMorning Report 11 JuliI Wayan ArimbawaNoch keine Bewertungen
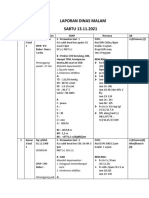
- Laporan Dinas Malam.13.11.21 MiaDokument9 SeitenLaporan Dinas Malam.13.11.21 Miayuni hunainiNoch keine Bewertungen
- Leaflet Daire 2Dokument2 SeitenLeaflet Daire 2Nitha KoliNoch keine Bewertungen
- Cover LapsusDokument1 SeiteCover LapsusNitha KoliNoch keine Bewertungen
- Leaflet Daire 2Dokument2 SeitenLeaflet Daire 2Nitha KoliNoch keine Bewertungen
- Lamp IranDokument1 SeiteLamp IranNitha KoliNoch keine Bewertungen
- Morning Report 2Dokument10 SeitenMorning Report 2Nitha KoliNoch keine Bewertungen
- Surgical Sutures and NeedlesDokument39 SeitenSurgical Sutures and NeedlesNitha KoliNoch keine Bewertungen
- An Update On The Pathogenesis of DiabetesDokument12 SeitenAn Update On The Pathogenesis of DiabetesAmalia Elena BulanceaNoch keine Bewertungen
- Ar Statement Vita Permai Feb'15Dokument2 SeitenAr Statement Vita Permai Feb'15Nitha KoliNoch keine Bewertungen
- Tenggam Nmur - Sfbjaffljh Taip /FD: Llim Tdi, Ilknnt, - Ts Jer SLCLRNH @.Ht:-Nand Rt/Ryi' L1Artut Aoana:Elam RugdaDokument1 SeiteTenggam Nmur - Sfbjaffljh Taip /FD: Llim Tdi, Ilknnt, - Ts Jer SLCLRNH @.Ht:-Nand Rt/Ryi' L1Artut Aoana:Elam RugdaNitha KoliNoch keine Bewertungen
- Tenggam Nmur - Sfbjaffljh Taip /FD: Llim Tdi, Ilknnt, - Ts Jer SLCLRNH @.Ht:-Nand Rt/Ryi' L1Artut Aoana:Elam RugdaDokument1 SeiteTenggam Nmur - Sfbjaffljh Taip /FD: Llim Tdi, Ilknnt, - Ts Jer SLCLRNH @.Ht:-Nand Rt/Ryi' L1Artut Aoana:Elam RugdaNitha KoliNoch keine Bewertungen
- Abstract Skripsi Bahasa InggrisDokument1 SeiteAbstract Skripsi Bahasa InggrisNitha KoliNoch keine Bewertungen
- Bell - S Palsy Aetiology, Classification, Differential Diagnosis and Treatment Consideration A ReviewDokument8 SeitenBell - S Palsy Aetiology, Classification, Differential Diagnosis and Treatment Consideration A ReviewekramsNoch keine Bewertungen
- Bell - S Palsy Aetiology, Classification, Differential Diagnosis and Treatment Consideration A ReviewDokument8 SeitenBell - S Palsy Aetiology, Classification, Differential Diagnosis and Treatment Consideration A ReviewekramsNoch keine Bewertungen