Das könnte Ihnen auch gefallen
- Self Doc AttestDokument1 SeiteSelf Doc Attestone twoNoch keine Bewertungen
- 6-Month Usmle Step 1 Sample Schedule Day Event Subjects Pathoma TasksDokument15 Seiten6-Month Usmle Step 1 Sample Schedule Day Event Subjects Pathoma Tasksone twoNoch keine Bewertungen
- Ecfmg: Information BookletDokument50 SeitenEcfmg: Information Bookletone twoNoch keine Bewertungen
- Fees For Consular Services RevisedDokument1 SeiteFees For Consular Services Revisedone twoNoch keine Bewertungen
- Form 900Dokument1 SeiteForm 900one twoNoch keine Bewertungen
- Manish Khanal Mobile: 9841842618Dokument1 SeiteManish Khanal Mobile: 9841842618one twoNoch keine Bewertungen
- Curriculum Vitae: Sagar KhadkaDokument2 SeitenCurriculum Vitae: Sagar Khadkaone twoNoch keine Bewertungen
- National Institute of Neurological and Heart Center Pvt. Ltd. Kathmandu, NepalDokument7 SeitenNational Institute of Neurological and Heart Center Pvt. Ltd. Kathmandu, Nepalone twoNoch keine Bewertungen
- .:ftyafrsqm Rqidq, T Ffiq ,"R.: (@N. (O9Blobz,)Dokument4 Seiten.:ftyafrsqm Rqidq, T Ffiq ,"R.: (@N. (O9Blobz,)one twoNoch keine Bewertungen
- Sujan Lal TamangDokument5 SeitenSujan Lal Tamangone twoNoch keine Bewertungen
- Bidwata Rai Khumltar, Lalitpur, Nepal Contact No.: 9869075699 EmailDokument2 SeitenBidwata Rai Khumltar, Lalitpur, Nepal Contact No.: 9869075699 Emailone twoNoch keine Bewertungen
- Sarmila CVDokument1 SeiteSarmila CVone twoNoch keine Bewertungen
- Curriculum Vitae of Ms. Pushpa SharmaDokument4 SeitenCurriculum Vitae of Ms. Pushpa Sharmaone twoNoch keine Bewertungen
- Yeti Health Science Academy Purbanchal University Kantimarg, KathmanduDokument104 SeitenYeti Health Science Academy Purbanchal University Kantimarg, Kathmanduone twoNoch keine Bewertungen
- Tender 30 075 076 Maintenance Items BOQDokument10 SeitenTender 30 075 076 Maintenance Items BOQone twoNoch keine Bewertungen
- TOR For Building DesignDokument2 SeitenTOR For Building Designone twoNoch keine Bewertungen
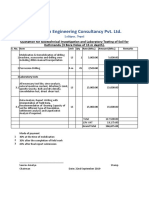
- Quotation For Soil TestDokument1 SeiteQuotation For Soil Testone twoNoch keine Bewertungen
- PKC and AssociatesDokument4 SeitenPKC and Associatesone twoNoch keine Bewertungen
- SFDBF/X?SF Nflu Yk TFNLD: Lbuf) Tyf DDFLGT /F) Huf/Lsf Nflu LK Kl/Of) HGFSF) Sfo (QMD Cgtu (TDokument5 SeitenSFDBF/X?SF Nflu Yk TFNLD: Lbuf) Tyf DDFLGT /F) Huf/Lsf Nflu LK Kl/Of) HGFSF) Sfo (QMD Cgtu (Tone twoNoch keine Bewertungen
- Staff QualificationvvvvvDokument12 SeitenStaff Qualificationvvvvvone twoNoch keine Bewertungen
- Nepal Medical Council: Application Form For Eligibility Certificate ForDokument5 SeitenNepal Medical Council: Application Form For Eligibility Certificate Forone twoNoch keine Bewertungen
- Physiological Anatomy of Respiratory Tract: Normal Respiratory Rate at Different AgeDokument1 SeitePhysiological Anatomy of Respiratory Tract: Normal Respiratory Rate at Different Ageone twoNoch keine Bewertungen
- Tribhuwan University Institute of Medicine Nepalgunj Nursing Campus Bns ProgrammeDokument76 SeitenTribhuwan University Institute of Medicine Nepalgunj Nursing Campus Bns Programmeone twoNoch keine Bewertungen
- Leadership and MGMT ReportDokument9 SeitenLeadership and MGMT Reportone twoNoch keine Bewertungen
- Institute of Postgraduate and Continuous Education For Post Graduation Study inDokument1 SeiteInstitute of Postgraduate and Continuous Education For Post Graduation Study inone twoNoch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Jurnal 2Dokument0 SeitenJurnal 2Seftiana SaftariNoch keine Bewertungen
- Indra Nooyi Draws On Vision and Values To LeadDokument1 SeiteIndra Nooyi Draws On Vision and Values To Leadimrul khanNoch keine Bewertungen
- ProjectDokument3 SeitenProjectAnshul PaunikarNoch keine Bewertungen
- Sfsac@xmu - Edu.my: To: From: FIS1012050@. Xmu - Edu.my Subject: Concern of Final Examination Amid Covid-19Dokument2 SeitenSfsac@xmu - Edu.my: To: From: FIS1012050@. Xmu - Edu.my Subject: Concern of Final Examination Amid Covid-19Ahmad RazaNoch keine Bewertungen
- Viral Exanthem ManagementDokument4 SeitenViral Exanthem Managementrona ellein galoNoch keine Bewertungen
- Homoeopathic Drug Pictures PDFDokument718 SeitenHomoeopathic Drug Pictures PDFNimesh PatelNoch keine Bewertungen
- A Clinal Primer On Intellectual DisabilityDokument13 SeitenA Clinal Primer On Intellectual DisabilityAra AzzahraNoch keine Bewertungen
- Haad QuestionDokument20 SeitenHaad QuestionNimraj PatelNoch keine Bewertungen
- Respiratory Support in ChildDokument8 SeitenRespiratory Support in ChildHưng TrầnNoch keine Bewertungen
- Drugs Used in IBDDokument44 SeitenDrugs Used in IBDBegmuhammet BabayevNoch keine Bewertungen
- Labs and NCP #2Dokument3 SeitenLabs and NCP #2Yen Valien CugayNoch keine Bewertungen
- Sample Outline AntibioticsDokument4 SeitenSample Outline AntibioticsNAPIZEVANSNoch keine Bewertungen
- Common Health Problems of Infancy PowptDokument78 SeitenCommon Health Problems of Infancy PowptCiella Dela CruzNoch keine Bewertungen
- Chest Physician in Pune - Dr. Sharadchandra YadavDokument8 SeitenChest Physician in Pune - Dr. Sharadchandra YadavSharad YadavNoch keine Bewertungen
- 2.1 NCM 109 - Pregestational ConditionsDokument6 Seiten2.1 NCM 109 - Pregestational ConditionsSittie Haneen TabaraNoch keine Bewertungen
- Chapter 42 - GastroenteritisDokument17 SeitenChapter 42 - GastroenteritiskafosidNoch keine Bewertungen
- Grade 5 Term 4 Life Skills Lesson Plan Name of Lesson: Become A Disease Detective!Dokument3 SeitenGrade 5 Term 4 Life Skills Lesson Plan Name of Lesson: Become A Disease Detective!Raeesa SNoch keine Bewertungen
- Weight Loss and Wasting SyndromeDokument4 SeitenWeight Loss and Wasting Syndromeeel100% (1)
- 2007Dokument6 Seiten2007api-302133133Noch keine Bewertungen
- Viva Questions DermatologyDokument5 SeitenViva Questions DermatologyRavva0% (1)
- Sexual HealthDokument11 SeitenSexual Healthapi-236516264Noch keine Bewertungen
- Buildings and Structures: Padua EsteDokument2 SeitenBuildings and Structures: Padua EsteKevin LavinaNoch keine Bewertungen
- Bhagatwala Et Al 2015, Indications and ContraindicationsDokument27 SeitenBhagatwala Et Al 2015, Indications and Contraindicationsedo adimastaNoch keine Bewertungen
- Polyarteritis NodosaDokument10 SeitenPolyarteritis Nodosaaaron mbindyoNoch keine Bewertungen
- Drug Study NCP - San LazaroDokument9 SeitenDrug Study NCP - San LazaroLynne CammayoNoch keine Bewertungen
- Activities-Specific Balance Confidence (Abc) ScaleDokument16 SeitenActivities-Specific Balance Confidence (Abc) ScaleMochammad Syarif HidayatNoch keine Bewertungen
- Newsletter: WHO PharmaceuticalsDokument27 SeitenNewsletter: WHO PharmaceuticalsGammachuu Leejjiisa Mul'ataa SabbooqaaNoch keine Bewertungen
- Role and Functions of Mental Health NurseDokument20 SeitenRole and Functions of Mental Health NurseBinal Joshi86% (7)
- Antibiotics CasesDokument39 SeitenAntibiotics CasesnistaneNoch keine Bewertungen