Das könnte Ihnen auch gefallen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5795)
- Asthma Broncial (Theophylline)Dokument41 SeitenAsthma Broncial (Theophylline)Nadya Zahra Henni100% (1)
- Pharmacokinetics VariabilityDokument21 SeitenPharmacokinetics VariabilityNadya Zahra HenniNoch keine Bewertungen
- Ekskresi Kel. 5Dokument22 SeitenEkskresi Kel. 5Nadya Zahra HenniNoch keine Bewertungen
- GLPDokument6 SeitenGLPNadya Zahra HenniNoch keine Bewertungen
- Topical Drug Classification PDFDokument12 SeitenTopical Drug Classification PDFNadya Zahra HenniNoch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Q.P. CODE:500-A-OR: BiochemistryDokument38 SeitenQ.P. CODE:500-A-OR: BiochemistrySai KiranNoch keine Bewertungen
- 2013 Pneumonia Due To Multidrug-Resistant Leclercia AdecarboxylataDokument3 Seiten2013 Pneumonia Due To Multidrug-Resistant Leclercia AdecarboxylataLexotanyl LexiNoch keine Bewertungen
- Pi Is 0002937808008806Dokument7 SeitenPi Is 0002937808008806venkayammaNoch keine Bewertungen
- Cisplatin ArticleDokument2 SeitenCisplatin ArticleImbsat HabibNoch keine Bewertungen
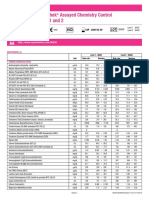
- Lyphochek Assayed Chemistry Control Levels 1 and 2: Siemens Dimension SeriesDokument2 SeitenLyphochek Assayed Chemistry Control Levels 1 and 2: Siemens Dimension SeriesAmie zulaikaNoch keine Bewertungen
- Acute Kidney Injury 2019Dokument16 SeitenAcute Kidney Injury 2019ShadowK 99Noch keine Bewertungen
- Laboratory and Diagnostic TestDokument3 SeitenLaboratory and Diagnostic TestKristine Artes AguilarNoch keine Bewertungen
- CANINE-Hematologic and Serum Biochemical Reference Values in Retired GreyhoundsDokument6 SeitenCANINE-Hematologic and Serum Biochemical Reference Values in Retired Greyhoundstaner_soysurenNoch keine Bewertungen
- Clearance and GFR: Major DR Arabinda Mohan Bhattarai Lecturer (Biochemistry), NAIHSDokument25 SeitenClearance and GFR: Major DR Arabinda Mohan Bhattarai Lecturer (Biochemistry), NAIHSChandan SahNoch keine Bewertungen
- Non-Protein Nitrogen Compounds1 (FINALS)Dokument60 SeitenNon-Protein Nitrogen Compounds1 (FINALS)Marydith Ortillo100% (1)
- Screenshot 2023-03-30 at 9.08.15 PMDokument14 SeitenScreenshot 2023-03-30 at 9.08.15 PMUrvi KaliaNoch keine Bewertungen
- Tickler PDFDokument177 SeitenTickler PDFQueenie FarrahNoch keine Bewertungen
- Anesthesia For Kidney DiseaseDokument6 SeitenAnesthesia For Kidney DiseaseFrits Dede SinagaNoch keine Bewertungen
- PCP in A Box - Module 2Dokument49 SeitenPCP in A Box - Module 2shaheershayanqaziNoch keine Bewertungen
- Terapi Farmakologi Pada GeriatriDokument42 SeitenTerapi Farmakologi Pada Geriatrielkhachank142Noch keine Bewertungen
- Creatine The Power Supplement LIVRODokument295 SeitenCreatine The Power Supplement LIVROAndré Codea100% (2)
- Chapter 11 - Drug Therapy in GeriatricsDokument4 SeitenChapter 11 - Drug Therapy in Geriatricsdlneisha61100% (1)
- Random Facts (Nclex Stuff)Dokument305 SeitenRandom Facts (Nclex Stuff)Jamielah Romano100% (9)
- Physiologic Monitoring of The Surgical PatientDokument56 SeitenPhysiologic Monitoring of The Surgical PatientSeid Adem100% (2)
- Test Bank For Nutrition Diet Therapy 10th Edition Ruth A RothDokument36 SeitenTest Bank For Nutrition Diet Therapy 10th Edition Ruth A Rothcurlerbedye7dlv100% (37)
- Guidelines For Laboratory Practice 2012 PDFDokument81 SeitenGuidelines For Laboratory Practice 2012 PDFMauricio Vanessa Juliana Koury PalmeiraNoch keine Bewertungen
- Neonatal Acute Kidney InjuryDokument58 SeitenNeonatal Acute Kidney InjuryRadhika BatraNoch keine Bewertungen
- Fenofibrate-Associated Nephrotoxicity: A Review of Current EvidenceDokument8 SeitenFenofibrate-Associated Nephrotoxicity: A Review of Current EvidencefevianaNoch keine Bewertungen
- Keto Acid Therapy in CKDDokument23 SeitenKeto Acid Therapy in CKDDrajad PriyonoNoch keine Bewertungen
- Creatinine ClearanceDokument6 SeitenCreatinine ClearancedianaNoch keine Bewertungen
- Stability of Selected Biochemical Analytes in Plasma Samples Stored Under Different Time and Temperature ConditionsDokument4 SeitenStability of Selected Biochemical Analytes in Plasma Samples Stored Under Different Time and Temperature ConditionsVincent ReyesNoch keine Bewertungen
- High Blood PressureDokument62 SeitenHigh Blood PressureF SupportNoch keine Bewertungen
- (CC1) LEC-W12-Nonprotein Nitrogen CompoundsDokument10 Seiten(CC1) LEC-W12-Nonprotein Nitrogen CompoundsAira UsiNoch keine Bewertungen
- Zomen in CKDDokument12 SeitenZomen in CKDClaudiu BalabanNoch keine Bewertungen
- Urine Protein andDokument12 SeitenUrine Protein andAfifah AzizNoch keine Bewertungen