Das könnte Ihnen auch gefallen
- Akne Vulgaris: Dr. Sani Widjaja, SP - KK Bag/SMF IK Kulit & Kelamin FK UNLAM/RSUD ULIN BanjarmasinDokument10 SeitenAkne Vulgaris: Dr. Sani Widjaja, SP - KK Bag/SMF IK Kulit & Kelamin FK UNLAM/RSUD ULIN BanjarmasinNanda SusiloNoch keine Bewertungen
- Refrat Daftar PusakaDokument2 SeitenRefrat Daftar PusakaNanda SusiloNoch keine Bewertungen
- CraniumDokument50 SeitenCraniumSyarifahUniqueNoch keine Bewertungen
- My Oath: By: Aditya Sanjaya 12DDokument1 SeiteMy Oath: By: Aditya Sanjaya 12DNanda SusiloNoch keine Bewertungen
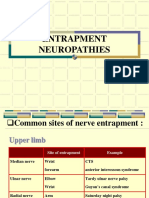
- ESSENTIAL GUIDE TO NERVE ENTRAPMENT NEUROPATHIESDokument15 SeitenESSENTIAL GUIDE TO NERVE ENTRAPMENT NEUROPATHIESNanda SusiloNoch keine Bewertungen
- Non Occupational CadmiumDokument10 SeitenNon Occupational CadmiumNanda SusiloNoch keine Bewertungen
- Environmental Exposure ToDokument9 SeitenEnvironmental Exposure ToNanda SusiloNoch keine Bewertungen
- Non Occupational CadmiumDokument10 SeitenNon Occupational CadmiumNanda SusiloNoch keine Bewertungen
- Early Versus Delayed Administration of Norepinephrine in Patients With Septic ShockDokument8 SeitenEarly Versus Delayed Administration of Norepinephrine in Patients With Septic ShockNanda SusiloNoch keine Bewertungen
- Lampiran 1. Surat Permohonan Kesediaan Menjadi Subjek PenelitianDokument9 SeitenLampiran 1. Surat Permohonan Kesediaan Menjadi Subjek PenelitianNanda SusiloNoch keine Bewertungen
- Bab IiDokument13 SeitenBab IiNanda SusiloNoch keine Bewertungen
- Kidney Cadmium Toxicity, Diabetes and High Blood Pressure: The Perfect StormDokument23 SeitenKidney Cadmium Toxicity, Diabetes and High Blood Pressure: The Perfect StormNanda SusiloNoch keine Bewertungen
- eTicket Itinerary Receipt for Domestic Lion Air FlightDokument2 SeiteneTicket Itinerary Receipt for Domestic Lion Air FlightTaufan RennaldyNoch keine Bewertungen
- A Trophozoite of Trichomonas Vaginalis From CultureDokument1 SeiteA Trophozoite of Trichomonas Vaginalis From CultureNanda SusiloNoch keine Bewertungen
- A Trophozoite of Trichomonas Vaginalis From CultureDokument1 SeiteA Trophozoite of Trichomonas Vaginalis From CultureNanda SusiloNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5782)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (72)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Children 09 00723Dokument7 SeitenChildren 09 00723radu nicolaeNoch keine Bewertungen
- SANGKULA Drug-Study-FormatDokument3 SeitenSANGKULA Drug-Study-FormatAnonymous p0DPE1eNoch keine Bewertungen
- Syllabus - M SC (Nursing)Dokument59 SeitenSyllabus - M SC (Nursing)chikitsakNoch keine Bewertungen
- Sai Vibrionics Newsletter From The Desk of DR Jit K AggarwalDokument18 SeitenSai Vibrionics Newsletter From The Desk of DR Jit K AggarwalSujok Swadesh100% (1)
- Community-Acquired Pneumoniaandhospital-Acquiredpneumonia: Charles W. Lanks,, Ali I. Musani,, David W. HsiaDokument15 SeitenCommunity-Acquired Pneumoniaandhospital-Acquiredpneumonia: Charles W. Lanks,, Ali I. Musani,, David W. HsiaMajo EscobarNoch keine Bewertungen
- Glass Ionomer Cement)Dokument1 SeiteGlass Ionomer Cement)Resa Dwi WNoch keine Bewertungen
- IBS and SIBO Differential Diagnosis, SiebeckerDokument1 SeiteIBS and SIBO Differential Diagnosis, SiebeckerKrishna DasNoch keine Bewertungen
- 6 HypertensionDokument95 Seiten6 HypertensionZeleke temechewNoch keine Bewertungen
- Possible Nursing Care Plan Assessment Need Nursing Diagnosis Objective of Care Nursing InterventionDokument12 SeitenPossible Nursing Care Plan Assessment Need Nursing Diagnosis Objective of Care Nursing InterventionClaire M. AuditorNoch keine Bewertungen
- ECG Basics for AnesthesiologistsDokument145 SeitenECG Basics for AnesthesiologistsKM Lakshmana RajanNoch keine Bewertungen
- Understanding Puerperal SepsisDokument22 SeitenUnderstanding Puerperal SepsisSuhas IngaleNoch keine Bewertungen
- Boswellia: An Evidence-Based Systematic Review by The Natural Standard Research CollaborationDokument21 SeitenBoswellia: An Evidence-Based Systematic Review by The Natural Standard Research CollaborationMichael Kohlberger, BSc MScNoch keine Bewertungen
- ანტიგენების პროცესინგი და პრეზენტაციაDokument1 Seiteანტიგენების პროცესინგი და პრეზენტაციაEMD GROUPNoch keine Bewertungen
- Atelectasis SymptomsDokument4 SeitenAtelectasis SymptomsMelDred Cajes BolandoNoch keine Bewertungen
- Microbiology MUHS Questions (2005-2015)Dokument4 SeitenMicrobiology MUHS Questions (2005-2015)Shahid KhanNoch keine Bewertungen
- A Doppler-Based Evaluation of Peripheral Lower Limb Arterial Insufficiency in Diabetes MellitusDokument4 SeitenA Doppler-Based Evaluation of Peripheral Lower Limb Arterial Insufficiency in Diabetes Mellitusresta_pxdNoch keine Bewertungen
- UrologyDokument5 SeitenUrologynice videosNoch keine Bewertungen
- In-House Canine and Feline Blood Typing: Bernard F. Feldman, DVM, PHD, VMRCVMDokument64 SeitenIn-House Canine and Feline Blood Typing: Bernard F. Feldman, DVM, PHD, VMRCVMtemplarioNoch keine Bewertungen
- Psych DrugsDokument12 SeitenPsych Drugsapi-3739910100% (1)
- Drug Study Batch 3 - Kristele Marie Joy CuaDokument26 SeitenDrug Study Batch 3 - Kristele Marie Joy CuaKristele Marie Joy CuaNoch keine Bewertungen
- Neonatal Seizures GuidelineDokument15 SeitenNeonatal Seizures GuidelineNURUL NADIA BINTI MOHD NAZIR / UPMNoch keine Bewertungen
- Coronary Artery Disease & Hypertension Practice Quiz (50 Questions)Dokument18 SeitenCoronary Artery Disease & Hypertension Practice Quiz (50 Questions)Erica Veluz LuyunNoch keine Bewertungen
- Carcinoma GasterDokument32 SeitenCarcinoma GasterAzhari AhsanNoch keine Bewertungen
- 5th Parkinson'sDokument736 Seiten5th Parkinson'sirfanifitriNoch keine Bewertungen
- Cardiac Five YearsDokument31 SeitenCardiac Five Yearsdileepkumar.duhs4817Noch keine Bewertungen
- Glaucoma, Hyphema: Synonyms and Related Keywords: Hyphema, Microhyphema, Hemorrhage in The AnteriorDokument22 SeitenGlaucoma, Hyphema: Synonyms and Related Keywords: Hyphema, Microhyphema, Hemorrhage in The AnteriorWulandari EmyNoch keine Bewertungen
- LECTURE NOTE ON ASTHMA-WPS OfficeDokument7 SeitenLECTURE NOTE ON ASTHMA-WPS OfficeNaija Nurses TVNoch keine Bewertungen
- My Exam, 16 JanDokument5 SeitenMy Exam, 16 JanWalid Sakr100% (1)
- Stom ProfileDokument71 SeitenStom ProfileStefan CretuNoch keine Bewertungen
- Snake Bite Viii SemDokument69 SeitenSnake Bite Viii SemKENEDYNoch keine Bewertungen