Das könnte Ihnen auch gefallen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Jamaophthalmology Biswas 2016 Oi 160055Dokument8 SeitenJamaophthalmology Biswas 2016 Oi 160055Ghalia HayetNoch keine Bewertungen
- APA Practice Guideline For The Treatment of Patients With Substance Use DisordersDokument276 SeitenAPA Practice Guideline For The Treatment of Patients With Substance Use DisordersRaja Ahmad Rusdan MusyawirNoch keine Bewertungen
- Haematology Paper 1 - Past PapersDokument9 SeitenHaematology Paper 1 - Past Papersmma1976100% (1)
- Che 225 Control of Communicable DiseasesDokument19 SeitenChe 225 Control of Communicable DiseasesAbdullahi Bashir SalisuNoch keine Bewertungen
- Catalog EME PHYSIO 2016 - ENGDokument88 SeitenCatalog EME PHYSIO 2016 - ENGaudrey pahleviNoch keine Bewertungen
- Axa Group Corporate PresentationDokument35 SeitenAxa Group Corporate PresentationRajneesh VermaNoch keine Bewertungen
- Lesson Plan On Spina BifidaDokument24 SeitenLesson Plan On Spina BifidaPriyaNoch keine Bewertungen
- TramadolDokument2 SeitenTramadolJordanne EtisNoch keine Bewertungen
- Endodontics Pain Control in Endodontics: Differential Diagnosis of Dental PainDokument4 SeitenEndodontics Pain Control in Endodontics: Differential Diagnosis of Dental Painريام الموسويNoch keine Bewertungen
- Bacteria Found in UrineDokument7 SeitenBacteria Found in UrineAria DomingoNoch keine Bewertungen
- Full Body To Body Massage Centre in MG Road Gurgaon - Spa in Gurgaon MG RoadDokument11 SeitenFull Body To Body Massage Centre in MG Road Gurgaon - Spa in Gurgaon MG RoadFlip Body SpaNoch keine Bewertungen
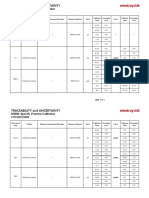
- Specific Proteins Calibrator-150721009-BS600Dokument2 SeitenSpecific Proteins Calibrator-150721009-BS600S6b2Noch keine Bewertungen
- Insights and Images: Vascular Channel Mimicking A Skull FractureDokument2 SeitenInsights and Images: Vascular Channel Mimicking A Skull Fracturethariq mubarakNoch keine Bewertungen
- AttachmentDokument39 SeitenAttachmentshmlniz100% (1)
- Diabetes Jigsaw ActivitiesDokument11 SeitenDiabetes Jigsaw ActivitiesJacqueline CullieNoch keine Bewertungen
- Behavioral Health Care Plan: Assessment DataDokument9 SeitenBehavioral Health Care Plan: Assessment Dataapi-521018364Noch keine Bewertungen
- The Role of Radiotherapy in Cancer TreatmentDokument9 SeitenThe Role of Radiotherapy in Cancer TreatmentarakbaeNoch keine Bewertungen
- Annotated BibliographyDokument4 SeitenAnnotated BibliographyJuanNoch keine Bewertungen
- Lipo LaserDokument13 SeitenLipo LaserLuis A Gil Pantoja100% (1)
- Feeling GreatDokument243 SeitenFeeling GreatSunny LamNoch keine Bewertungen
- Wards and Departments in The Hospital NamingDokument4 SeitenWards and Departments in The Hospital NamingSlebeww PetewNoch keine Bewertungen
- Exercise PrescriptionDokument53 SeitenExercise PrescriptionEvangeline A. Alegre100% (1)
- New TNMDokument157 SeitenNew TNMShouvik ChowdhuryNoch keine Bewertungen
- OS Pharmacy L III - IVDokument125 SeitenOS Pharmacy L III - IVashagrie67% (3)
- SP42 Thoracentesis (Adult)Dokument7 SeitenSP42 Thoracentesis (Adult)Adam HuzaibyNoch keine Bewertungen
- Ok - Effect of Melatonin On Broiler ChicksDokument12 SeitenOk - Effect of Melatonin On Broiler ChicksOliver TalipNoch keine Bewertungen
- Celiac DiseaseDokument35 SeitenCeliac DiseaseRye HanaNoch keine Bewertungen
- Hydatidiform MoleDokument2 SeitenHydatidiform MoleIrfan HardiNoch keine Bewertungen
- HIV Drug Chart (2021)Dokument1 SeiteHIV Drug Chart (2021)savNoch keine Bewertungen
- Assessment of Vital Signs&GCSDokument3 SeitenAssessment of Vital Signs&GCSNicole Jackson100% (3)