Das könnte Ihnen auch gefallen
- Hernia, (Different Types) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsVon EverandHernia, (Different Types) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsBewertung: 5 von 5 Sternen5/5 (1)
- Key PointsDokument34 SeitenKey PointsSe YunNoch keine Bewertungen
- Hernia Seminar 2 Aug 2014 FinalDokument20 SeitenHernia Seminar 2 Aug 2014 FinalKishan NaiduNoch keine Bewertungen
- GS2 HerniaDokument13 SeitenGS2 HerniaMAH pedNoch keine Bewertungen
- Intestinal Diseases, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsVon EverandIntestinal Diseases, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNoch keine Bewertungen
- Hernia: DR - Surender Singh DhankharDokument36 SeitenHernia: DR - Surender Singh DhankharBharat BhushanNoch keine Bewertungen
- A Manual of the Operations of Surgery: For the Use of Senior Students, House Surgeons, and Junior PractitionersVon EverandA Manual of the Operations of Surgery: For the Use of Senior Students, House Surgeons, and Junior PractitionersNoch keine Bewertungen
- AbdWall, Hernia Atbp - AnnoDokument34 SeitenAbdWall, Hernia Atbp - AnnoJuan Lorenzo RequironNoch keine Bewertungen
- Impression HerniaDokument3 SeitenImpression Herniakjeseo8Noch keine Bewertungen
- Hernia IngunalisDokument29 SeitenHernia Ingunalisyaodoe1Noch keine Bewertungen
- CSS Hernia Inguinalis - SalmaDokument28 SeitenCSS Hernia Inguinalis - SalmaNamira PutriNoch keine Bewertungen
- Open Inguinal Hernia RepairDokument6 SeitenOpen Inguinal Hernia RepairKris TejereroNoch keine Bewertungen
- Abdominal HerniasDokument38 SeitenAbdominal HerniasHafizah HoshniNoch keine Bewertungen
- Anatomy of Inguinal CanalDokument10 SeitenAnatomy of Inguinal CanalsaisoniaNoch keine Bewertungen
- Hernias: General Features To All Types of HerniasDokument19 SeitenHernias: General Features To All Types of Herniashussain AltaherNoch keine Bewertungen
- Hernia: Done by D1 GroupDokument47 SeitenHernia: Done by D1 Groupanindyadputri100% (1)
- The Abdominal WallDokument32 SeitenThe Abdominal WallarshmeentariqNoch keine Bewertungen
- HerniaDokument46 SeitenHerniaZubairkhan SuraniNoch keine Bewertungen
- Lo 5Dokument13 SeitenLo 5Mutiara Prima DianaNoch keine Bewertungen
- HerniaDokument47 SeitenHerniamalathiNoch keine Bewertungen
- Pared Abdominal Hernia 1Dokument39 SeitenPared Abdominal Hernia 1Florentino EspitiaNoch keine Bewertungen
- Hernia Scrotalis FIxDokument56 SeitenHernia Scrotalis FIxivaniNoch keine Bewertungen
- Perineal HerniaDokument3 SeitenPerineal Herniagogovet101Noch keine Bewertungen
- Abdominal Wall and HerniaDokument35 SeitenAbdominal Wall and HerniaMohammad BanisalmanNoch keine Bewertungen
- Ventral HerniaDokument29 SeitenVentral HerniaNamerahNNoch keine Bewertungen
- PERINEUMDokument24 SeitenPERINEUMmhr27112002Noch keine Bewertungen
- HerniaDokument3 SeitenHerniadNoch keine Bewertungen
- Abdomen MCQDokument24 SeitenAbdomen MCQTatyanna Rammouz100% (1)
- 13 Genital Tract InjuriesDokument100 Seiten13 Genital Tract InjuriesRana Vandana100% (1)
- HerniaDokument67 SeitenHerniaياسر نعيم الربيعي100% (1)
- U Michigan Written Quiz - Inguinal RegionDokument14 SeitenU Michigan Written Quiz - Inguinal Regiontheintrepiddodger0% (1)
- Hernia SanaDokument57 SeitenHernia SanaBurhanuddin BhindarwalaNoch keine Bewertungen
- Inguinal Hernias and Abdominal Wall Defects: Murad Nuserat & Abd AL-Rahman AlhelwDokument51 SeitenInguinal Hernias and Abdominal Wall Defects: Murad Nuserat & Abd AL-Rahman AlhelwRashed ShatnawiNoch keine Bewertungen
- HerniaDokument6 SeitenHerniavidro alifNoch keine Bewertungen
- Femoral HerniaDokument4 SeitenFemoral HerniaKatie AndersonNoch keine Bewertungen
- HerniaDokument106 SeitenHerniaDr-Mohammad Ali-Fayiz Al TamimiNoch keine Bewertungen
- Inguinal CanalDokument48 SeitenInguinal CanalMahi100% (1)
- Hernia1 InguinalDokument7 SeitenHernia1 InguinalmunafalmahdiNoch keine Bewertungen
- Wa0000. 1Dokument41 SeitenWa0000. 1Aditya SinghNoch keine Bewertungen
- Abdominal WallDokument75 SeitenAbdominal WallJojo RyelciusNoch keine Bewertungen
- Inguinal and Femoral HerniaDokument50 SeitenInguinal and Femoral HerniaFafa NabihaNoch keine Bewertungen
- HerniaDokument26 SeitenHerniaSudhanshu ShekharNoch keine Bewertungen
- Groin Hernias: Vic V. Vernenkar, D.O. St. Barnabas Hospital Bronx, NYDokument39 SeitenGroin Hernias: Vic V. Vernenkar, D.O. St. Barnabas Hospital Bronx, NYMuhammad Waqar UlfatNoch keine Bewertungen
- Inguinal HerniaDokument33 SeitenInguinal Herniatianally100% (2)
- HerniaDokument100 SeitenHerniaangelaanapaku100% (3)
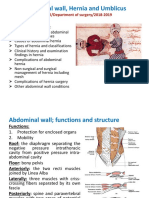
- Abdominal Wall, Hernia and Umblicus: M Kamil/Department of Surgery/2018-2019Dokument46 SeitenAbdominal Wall, Hernia and Umblicus: M Kamil/Department of Surgery/2018-2019AmmarNoch keine Bewertungen
- Hernias: Daniel IgoDokument46 SeitenHernias: Daniel Igobigboss80s100% (1)
- HERNIADokument8 SeitenHERNIArazan.girl.2010Noch keine Bewertungen
- Classification & Investigations of HerniaDokument56 SeitenClassification & Investigations of HerniaFobin VargheseNoch keine Bewertungen
- Anatomy of GIT For PCII Students..Dokument106 SeitenAnatomy of GIT For PCII Students..AMANUEL HABTEWOLDNoch keine Bewertungen
- Dinding Abdomen PSIKDokument79 SeitenDinding Abdomen PSIKSondang DamanikNoch keine Bewertungen
- 2nd Year All Clinicals AIMC AcademiaDokument64 Seiten2nd Year All Clinicals AIMC Academiasaleempanwar96Noch keine Bewertungen
- Abdominal HerniasDokument33 SeitenAbdominal Herniastianally100% (2)
- Types of Hernia and Its ManagementDokument80 SeitenTypes of Hernia and Its ManagementVisaagan Kalaithasan50% (2)
- Abdomen (Inguinal Hernia) : Anatomy II Block 3 NotesDokument39 SeitenAbdomen (Inguinal Hernia) : Anatomy II Block 3 NotesJoseph KimNoch keine Bewertungen
- Disusun Oleh:: Si Putu Agung Ratih S D 1765050364 Dr. Ade Hanny Kainama, SP BDokument40 SeitenDisusun Oleh:: Si Putu Agung Ratih S D 1765050364 Dr. Ade Hanny Kainama, SP BagungratihsdNoch keine Bewertungen
- OP Sliding & Strangulated Hernia & OrchiectomyDokument8 SeitenOP Sliding & Strangulated Hernia & OrchiectomyDeepika ChaudharyNoch keine Bewertungen
- Hernia Refarat Khansa 2Dokument31 SeitenHernia Refarat Khansa 2Khansa Hanifah Mutia100% (1)
- LP. Nr.3 - Dr. IspasDokument4 SeitenLP. Nr.3 - Dr. Ispasinna3003Noch keine Bewertungen
- LP - nr.2-dr. Ispas The Columna Vertebralis: The Corpus Vertebrae (Vertebral Body) Possesses An Upper and A Lower SurfaceDokument7 SeitenLP - nr.2-dr. Ispas The Columna Vertebralis: The Corpus Vertebrae (Vertebral Body) Possesses An Upper and A Lower Surfaceinna3003Noch keine Bewertungen
- The Occipital BoneDokument5 SeitenThe Occipital Boneinna3003Noch keine Bewertungen
- LungsDokument6 SeitenLungsinna3003Noch keine Bewertungen
- FCR Capsula Xl2 Brochure 01Dokument3 SeitenFCR Capsula Xl2 Brochure 01Zhandra50% (2)
- Reading ComprehensionDokument27 SeitenReading ComprehensionNguyen MinhNoch keine Bewertungen
- 9 ThalamusDokument10 Seiten9 ThalamusZoya MoraniNoch keine Bewertungen
- Thesis Statement Anxiety DisorderDokument8 SeitenThesis Statement Anxiety Disorderanneryssanchezpaterson100% (2)
- Portfolio COM3702Dokument42 SeitenPortfolio COM3702yog devi67% (9)
- Dissertation Nutrition PDFDokument8 SeitenDissertation Nutrition PDFWhoWillWriteMyPaperForMeUK100% (1)
- Intestinal Mucosal Barrier & Highly Absorptive CellsDokument25 SeitenIntestinal Mucosal Barrier & Highly Absorptive Cellsas qw100% (1)
- Gouty PowerpointDokument14 SeitenGouty PowerpointBSN4ANoch keine Bewertungen
- Hema 2 5th Ed SummaryDokument9 SeitenHema 2 5th Ed Summarymonzon.mika1801Noch keine Bewertungen
- Urea Plant Nangal 2014Dokument8 SeitenUrea Plant Nangal 2014Ishan HaiderNoch keine Bewertungen
- Diabetes Mellitus Surgical PatientDokument33 SeitenDiabetes Mellitus Surgical PatientGerald AndersonNoch keine Bewertungen
- Lecture On PHYSIOLOGY of Cerebellum by Dr. RoomiDokument42 SeitenLecture On PHYSIOLOGY of Cerebellum by Dr. RoomiMudassar Roomi100% (2)
- NCP EpilepsyDokument1 SeiteNCP EpilepsyManpreet ToorNoch keine Bewertungen
- CPE239 Demonstration 411Dokument11 SeitenCPE239 Demonstration 411Hong Jun TeeNoch keine Bewertungen
- Guardian Health & Life Insurance FormDokument2 SeitenGuardian Health & Life Insurance Formsmbdy tbhhhNoch keine Bewertungen
- Fiitjee: Talent Reward Exam - 2020Dokument25 SeitenFiitjee: Talent Reward Exam - 2020Imtesalur Rahman100% (1)
- Biology of Sars-Cov-2Dokument4 SeitenBiology of Sars-Cov-2J. L.Noch keine Bewertungen
- Obsessive-Compulsive Disorder (OCD) : Pop Ariana Narcisa Class XI-B Colegiul Tehnic Ana AslanDokument12 SeitenObsessive-Compulsive Disorder (OCD) : Pop Ariana Narcisa Class XI-B Colegiul Tehnic Ana AslanAriPopNoch keine Bewertungen
- FITT 2 (Midterm)Dokument13 SeitenFITT 2 (Midterm)CJyn PascualNoch keine Bewertungen
- INS452 Group - AssgmntDokument15 SeitenINS452 Group - Assgmntrienahsanari99Noch keine Bewertungen
- ! National MGMA Benchmarks - 2019 12Dokument5 Seiten! National MGMA Benchmarks - 2019 12unanda100% (1)
- Program and Proceedings - 8th International Neuroscience and Biological Psychiatry Regional ISBS Conference "STRESS AND BEHAVIOR: YOKOHAMA-2016", July 23-25, 2016, Yokohama, JapanDokument31 SeitenProgram and Proceedings - 8th International Neuroscience and Biological Psychiatry Regional ISBS Conference "STRESS AND BEHAVIOR: YOKOHAMA-2016", July 23-25, 2016, Yokohama, JapanISBS_SocietyNoch keine Bewertungen
- Pharma Mar Smart Fund Short ThesisDokument24 SeitenPharma Mar Smart Fund Short Thesisjulia skripka-serry20% (5)
- Apraxia 2Dokument25 SeitenApraxia 2Vellardo AlbayNoch keine Bewertungen
- Eucalyptol Safety and Pharmacological ProfileDokument8 SeitenEucalyptol Safety and Pharmacological ProfileTim ThomasNoch keine Bewertungen
- Quitting Smoking Journal by Clear MindsDokument24 SeitenQuitting Smoking Journal by Clear MindsRajdeep MukherjeeNoch keine Bewertungen
- Health Claim FormDokument4 SeitenHealth Claim Formpandya hemangNoch keine Bewertungen
- Isoniazid TuberculosisDokument10 SeitenIsoniazid TuberculosisAisyah Aftita KamrasyidNoch keine Bewertungen
- Stress PDFDokument7 SeitenStress PDFGyanbitt KarNoch keine Bewertungen
- My Sister's Keeper Book ReviewDokument18 SeitenMy Sister's Keeper Book ReviewAnna KhayalanNoch keine Bewertungen