Das könnte Ihnen auch gefallen
- Virology:: Introduction To Virology, Its' Pathogenesis & EradicationDokument72 SeitenVirology:: Introduction To Virology, Its' Pathogenesis & EradicationAndi IrgiNoch keine Bewertungen
- Agglutination, Complement, Neutralization, and Inhibition: Methods in Immunology and Immunochemistry, Vol. 4Von EverandAgglutination, Complement, Neutralization, and Inhibition: Methods in Immunology and Immunochemistry, Vol. 4Noch keine Bewertungen
- VirologyDokument24 SeitenVirologyRohama Qubra 279Noch keine Bewertungen
- Pathogenesis of Viral InfectionsDokument13 SeitenPathogenesis of Viral InfectionsCitoy BastianNoch keine Bewertungen
- Medically Important VirusesDokument3 SeitenMedically Important Virusesgiannpee100% (1)
- Shanghai Medical Virology DepartmentDokument131 SeitenShanghai Medical Virology DepartmentvaidyamNoch keine Bewertungen
- Para, Viro MCQDokument63 SeitenPara, Viro MCQFitz Gerald CastilloNoch keine Bewertungen
- Viral Basics and Replication CyclesDokument21 SeitenViral Basics and Replication CyclesfrabziNoch keine Bewertungen
- 5 Basic VirologyDokument71 Seiten5 Basic VirologyErdemNoch keine Bewertungen
- Myxoviruses: MIDTERM LESSON 2: Respiratory VirusesDokument8 SeitenMyxoviruses: MIDTERM LESSON 2: Respiratory VirusesAnya IgnacioNoch keine Bewertungen
- Clinical VirologyDokument31 SeitenClinical VirologySally ElhadadNoch keine Bewertungen
- Part 2 of Medical VirologyDokument113 SeitenPart 2 of Medical Virologygatete samNoch keine Bewertungen
- Test Bank Exam 3Dokument81 SeitenTest Bank Exam 3Sajjad AhmadNoch keine Bewertungen
- Pathogenic Cocci Classification and CharacteristicsDokument72 SeitenPathogenic Cocci Classification and CharacteristicsManisanthosh KumarNoch keine Bewertungen
- The Medically Important MycosesDokument8 SeitenThe Medically Important MycosesNatasha JeanNoch keine Bewertungen
- Appropriate Clinical Specimens Collection and Transport For Diagnostic VirologyDokument48 SeitenAppropriate Clinical Specimens Collection and Transport For Diagnostic Virologylong thomNoch keine Bewertungen
- DNA Enveloped Viruses: Herpes VirusesDokument42 SeitenDNA Enveloped Viruses: Herpes VirusesUsman Ali AkbarNoch keine Bewertungen
- Viral (Aseptic) Meningitis) Main Cause of Common ColdDokument4 SeitenViral (Aseptic) Meningitis) Main Cause of Common ColdKatie Anne SaylerNoch keine Bewertungen
- Chapter II VirologyDokument116 SeitenChapter II VirologyTofikNoch keine Bewertungen
- Viral ReplicationDokument1 SeiteViral ReplicationMoh'd Ghanayem100% (1)
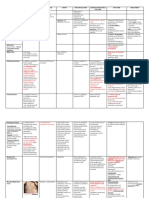
- Tables VirusesDokument9 SeitenTables VirusesOmphile DansonNoch keine Bewertungen
- VIRAL-DeTECTION Dxvirology AacbungayDokument102 SeitenVIRAL-DeTECTION Dxvirology AacbungayDominic Bernardo100% (1)
- CampylobacterDokument2 SeitenCampylobactersarguss14Noch keine Bewertungen
- 15medically Important Viruses PDFDokument75 Seiten15medically Important Viruses PDFdan ghaNoch keine Bewertungen
- Medical MycologyDokument14 SeitenMedical Mycologyhawkar omerNoch keine Bewertungen
- Viruses: Shafie Abdulkadir HassanDokument29 SeitenViruses: Shafie Abdulkadir HassanShafici CqadirNoch keine Bewertungen
- Human Immunodeficiency Virus InfectionDokument20 SeitenHuman Immunodeficiency Virus InfectionFatos ShuliNoch keine Bewertungen
- 27 MycologyDokument55 Seiten27 MycologyStephen Jao Ayala UjanoNoch keine Bewertungen
- Aerobic Non-Spore Forming Gram-Positive BacilliDokument31 SeitenAerobic Non-Spore Forming Gram-Positive BacilliCagar Irwin TaufanNoch keine Bewertungen
- Introduction To VirologyDokument55 SeitenIntroduction To VirologymulatumeleseNoch keine Bewertungen
- Subcutaneous MycosesDokument22 SeitenSubcutaneous MycosesCut Raihan100% (1)
- Agents of Mycoses Identification and CharacteristicsDokument44 SeitenAgents of Mycoses Identification and CharacteristicsRia AlcantaraNoch keine Bewertungen
- Cultivation of VirusDokument11 SeitenCultivation of VirusSUTHAN50% (2)
- Systemic MycosisDokument42 SeitenSystemic Mycosistummalapalli venkateswara raoNoch keine Bewertungen
- BunyaviridaeDokument12 SeitenBunyaviridaeRia AlcantaraNoch keine Bewertungen
- Microbiology MnemonicsDokument5 SeitenMicrobiology MnemonicsFritzel SusbillaNoch keine Bewertungen
- Immunology & Serology Week 1Dokument2 SeitenImmunology & Serology Week 1Romie SolacitoNoch keine Bewertungen
- Aerobic Gram PositiveDokument14 SeitenAerobic Gram PositiveMickey mg100% (1)
- General Virology 3.doc - 0Dokument14 SeitenGeneral Virology 3.doc - 0Isak Isak IsakNoch keine Bewertungen
- Answers To Virology MCQ Paper 2Dokument8 SeitenAnswers To Virology MCQ Paper 2Idrissa ContehNoch keine Bewertungen
- Virion, Virus, VirusoidDokument7 SeitenVirion, Virus, VirusoidGardina Erpe SiegarfieldNoch keine Bewertungen
- Family of StreptococcaceaeDokument10 SeitenFamily of StreptococcaceaeLovely B. AlipatNoch keine Bewertungen
- Classification of VirusesDokument39 SeitenClassification of VirusesYeyeh Santos100% (3)
- Foundations in Microbiology: TalaroDokument50 SeitenFoundations in Microbiology: Talaromertx013Noch keine Bewertungen
- Key elements of viruses and viral infectionsDokument44 SeitenKey elements of viruses and viral infectionsMay BerNoch keine Bewertungen
- AUBF Finals Vaginal SecretionsDokument37 SeitenAUBF Finals Vaginal SecretionsLyra Dennise LlidoNoch keine Bewertungen
- Virology Notes (RNA Virus)Dokument2 SeitenVirology Notes (RNA Virus)Mary Christelle100% (1)
- Mycology and VirologyDokument8 SeitenMycology and VirologyMaybelle Acap PatnubayNoch keine Bewertungen
- Basic Diagnostic Medical VirologyDokument31 SeitenBasic Diagnostic Medical VirologykashanNoch keine Bewertungen
- Virology LectureDokument16 SeitenVirology LectureJuan UmiwasNoch keine Bewertungen
- Papovaviridae PowerpointDokument53 SeitenPapovaviridae PowerpointMia Fernandez100% (3)
- Virology Sample Questions 1Dokument4 SeitenVirology Sample Questions 1William BufNoch keine Bewertungen
- MEDICAL VIROLOGY: VIRUSES CAN BE USEFULDokument82 SeitenMEDICAL VIROLOGY: VIRUSES CAN BE USEFULBaydaa Hameed Al Abdali100% (1)
- Virology NotesDokument81 SeitenVirology NotesraulNoch keine Bewertungen
- Leptospires General Characteristics:: Bacteriology: SpirochetesDokument5 SeitenLeptospires General Characteristics:: Bacteriology: SpirochetesJaellah MatawaNoch keine Bewertungen
- Medical MycologyDokument1 SeiteMedical MycologyHairul AnuarNoch keine Bewertungen
- 2.medical HelminthologyDokument148 Seiten2.medical HelminthologyHanifatur Rohmah100% (2)
- Mycology: Rochelle D. Darlucio-Yabut, RMT, MPH Our Lady of Fatima University College of Medical Laboratory ScienceDokument59 SeitenMycology: Rochelle D. Darlucio-Yabut, RMT, MPH Our Lady of Fatima University College of Medical Laboratory ScienceClaire GonoNoch keine Bewertungen
- Name: Reg No: Year: Branch: Course Name: Course Code: Title of SeminarDokument10 SeitenName: Reg No: Year: Branch: Course Name: Course Code: Title of SeminarKistoNoch keine Bewertungen
- DesignDokument1 SeiteDesignRod PasionNoch keine Bewertungen
- The Impact of Study Habits On The AcademDokument13 SeitenThe Impact of Study Habits On The AcademJames Fisc AndalesNoch keine Bewertungen
- Ra 544 - Ce LawDokument17 SeitenRa 544 - Ce LawRachelle C. Abanes100% (22)
- Must Know Parasitology TermsDokument22 SeitenMust Know Parasitology TermsvillajanellaNoch keine Bewertungen
- ER 2006-04 - Q2 ER - Infrastructure Spending and Philippine Development PDFDokument13 SeitenER 2006-04 - Q2 ER - Infrastructure Spending and Philippine Development PDFRod PasionNoch keine Bewertungen
- Matrix MethodDokument8 SeitenMatrix MethodRod PasionNoch keine Bewertungen
- Grade Control StructuresDokument7 SeitenGrade Control StructuresRod PasionNoch keine Bewertungen
- FLUID MECHANICS PROBLEM SETDokument5 SeitenFLUID MECHANICS PROBLEM SETKhale Kyrzhal RamirezNoch keine Bewertungen
- 10 1 1 544 1377 PDFDokument41 Seiten10 1 1 544 1377 PDFRod PasionNoch keine Bewertungen
- Node and element data for beam structureDokument24 SeitenNode and element data for beam structureRod PasionNoch keine Bewertungen
- Ass QH, Prob 3.2Dokument2 SeitenAss QH, Prob 3.2Rod PasionNoch keine Bewertungen
- The Impact of Study Habits On The AcademDokument21 SeitenThe Impact of Study Habits On The AcademRod PasionNoch keine Bewertungen
- Description:: Hydro 1 - HydrologyDokument55 SeitenDescription:: Hydro 1 - HydrologyRod PasionNoch keine Bewertungen
- Consider Et IonsDokument3 SeitenConsider Et IonsRod PasionNoch keine Bewertungen
- Specifications Heavy TimberDokument4 SeitenSpecifications Heavy TimberRod PasionNoch keine Bewertungen
- Specifications Heavy TimberDokument4 SeitenSpecifications Heavy TimberRod PasionNoch keine Bewertungen
- Materials Exam ReviewerDokument88 SeitenMaterials Exam ReviewerRod PasionNoch keine Bewertungen
- Computation of Average Rainfall Over A BasinDokument9 SeitenComputation of Average Rainfall Over A BasinEndless LoveNoch keine Bewertungen
- Medieval Philosophy: Key WordsDokument11 SeitenMedieval Philosophy: Key WordsRod PasionNoch keine Bewertungen
- Hematology Chemistry CoagulationDokument29 SeitenHematology Chemistry Coagulationdrafq2000Noch keine Bewertungen
- The Impact of Study Habits On The AcademDokument13 SeitenThe Impact of Study Habits On The AcademJames Fisc AndalesNoch keine Bewertungen
- The Impact of Study Habits On The AcademDokument13 SeitenThe Impact of Study Habits On The AcademJames Fisc AndalesNoch keine Bewertungen
- Criteria Selection For The Design of StructureDokument8 SeitenCriteria Selection For The Design of StructureRod PasionNoch keine Bewertungen
- Work Immersion CGDokument4 SeitenWork Immersion CGαλβιν δε100% (16)
- 2017MiniCalendar DawnNicoleDesigns PDFDokument12 Seiten2017MiniCalendar DawnNicoleDesigns PDFRod PasionNoch keine Bewertungen
- ColorWorksheets DawnNicoleDesignsDokument1 SeiteColorWorksheets DawnNicoleDesignsRod PasionNoch keine Bewertungen
- Thanks 5x7FoldedCard FullColor DawnNicoleDesignsDokument1 SeiteThanks 5x7FoldedCard FullColor DawnNicoleDesignsRod PasionNoch keine Bewertungen
- Thanks 5x7FoldedCard ColoringStyle DawnNicoleDesignsDokument1 SeiteThanks 5x7FoldedCard ColoringStyle DawnNicoleDesignsRod PasionNoch keine Bewertungen
- ColorWorksheets DawnNicoleDesigns PDFDokument11 SeitenColorWorksheets DawnNicoleDesigns PDFRod PasionNoch keine Bewertungen
- Insulators, Conductors and Semiconductors Classified by Energy Band StructureDokument1 SeiteInsulators, Conductors and Semiconductors Classified by Energy Band StructureRod PasionNoch keine Bewertungen
- EPIDEMIOLOGY and Plant Disease ForecastingDokument6 SeitenEPIDEMIOLOGY and Plant Disease Forecastingshyamsunder6850% (2)
- Community Health Nursing Doh Related Programs: Epi - Types of VaccinesDokument32 SeitenCommunity Health Nursing Doh Related Programs: Epi - Types of VaccinesAngelaNoch keine Bewertungen
- Pertussis CHN OutputDokument24 SeitenPertussis CHN OutputShannel J. DabalosNoch keine Bewertungen
- Wymowa - KopiaDokument2 SeitenWymowa - KopiaKinga DNoch keine Bewertungen
- Skripsi KustaDokument61 SeitenSkripsi Kustaandre yuindartantoNoch keine Bewertungen
- NipahDokument34 SeitenNipahpraisidNoch keine Bewertungen
- Waaw Posters PDFDokument4 SeitenWaaw Posters PDFRitna HaniNoch keine Bewertungen
- IN - AJA - Dazel Kit - Plan - V1 - 19042016Dokument16 SeitenIN - AJA - Dazel Kit - Plan - V1 - 19042016nagaraj2675Noch keine Bewertungen
- Malaria Presentation: Causes, Symptoms, TreatmentDokument23 SeitenMalaria Presentation: Causes, Symptoms, TreatmentAryan RajNoch keine Bewertungen
- 2nd Half Microbiology For Allied Health StudentsDokument404 Seiten2nd Half Microbiology For Allied Health StudentsFjornNoch keine Bewertungen
- CUPRINS1Dokument376 SeitenCUPRINS1Muntean MonicaNoch keine Bewertungen
- AAMC Immunization FormDokument4 SeitenAAMC Immunization FormJhalak AgrohiNoch keine Bewertungen
- 13 World Malaria DayDokument44 Seiten13 World Malaria DayMwanja MosesNoch keine Bewertungen
- Dip HIV Man (SA) Past Papers - 2012 Sept 15-5-2015Dokument3 SeitenDip HIV Man (SA) Past Papers - 2012 Sept 15-5-2015bkanoNoch keine Bewertungen
- Daftar PustakaDokument7 SeitenDaftar PustakaJonesius Eden ManoppoNoch keine Bewertungen
- Indian Baby Vaccination ChartDokument6 SeitenIndian Baby Vaccination ChartpramitaNoch keine Bewertungen
- Blood Donation Frequently Asked QuestionsDokument3 SeitenBlood Donation Frequently Asked QuestionsGrace ThairuNoch keine Bewertungen
- NPHL Test Handbook 2nd Edition 2022Dokument321 SeitenNPHL Test Handbook 2nd Edition 2022richmanchee23Noch keine Bewertungen
- Types of FeverDokument10 SeitenTypes of Fevermd191031Noch keine Bewertungen
- Lecture Eleven Prevention of HIV InfectionDokument8 SeitenLecture Eleven Prevention of HIV InfectionMaraka MichaelNoch keine Bewertungen
- Immunization & Pregnancy: Before During AfterDokument1 SeiteImmunization & Pregnancy: Before During Afterعمر وجدىNoch keine Bewertungen
- FCM 3 - 3A Group 8 - National AIDS STI Prevention and Control ProgramDokument184 SeitenFCM 3 - 3A Group 8 - National AIDS STI Prevention and Control ProgramRenz Francis SasaNoch keine Bewertungen
- D&D 5e SkavenDokument1 SeiteD&D 5e SkavensyNoch keine Bewertungen
- 7.systemic BacteriologyDokument88 Seiten7.systemic BacteriologyShimelis Teshome AyalnehNoch keine Bewertungen
- Certificate PDFDokument1 SeiteCertificate PDFKrupasham S JadhavNoch keine Bewertungen
- Prevalence of Syphilis Among Female Sex Workers and Their Clients in Togo in 2011Dokument5 SeitenPrevalence of Syphilis Among Female Sex Workers and Their Clients in Togo in 2011infokamarcewekNoch keine Bewertungen
- Modul-2 Pengobatan TB RO - Finished - 3112016 - TVDokument189 SeitenModul-2 Pengobatan TB RO - Finished - 3112016 - TVLasauva YardhaNoch keine Bewertungen
- Laboratory Diagnosis of MalariaDokument6 SeitenLaboratory Diagnosis of MalariaRam Sharma PaudelNoch keine Bewertungen
- Heron Herbals: Treating Lyme DiseaseDokument3 SeitenHeron Herbals: Treating Lyme DiseaseterryvndNoch keine Bewertungen
- Form Surv PD3IDokument5 SeitenForm Surv PD3Iluqyana fauzia hadiNoch keine Bewertungen