Das könnte Ihnen auch gefallen
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5795)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- IMMUNOLOGY AND SEROLOGY Exam Finalsb PDFDokument8 SeitenIMMUNOLOGY AND SEROLOGY Exam Finalsb PDFMarcelino CalataNoch keine Bewertungen
- Task 2 Case Notes: Brendan CrossDokument4 SeitenTask 2 Case Notes: Brendan Crossprakash poudelNoch keine Bewertungen
- How Important Is It For COVID Vaccine Distribution To Be Given With Equal AccessDokument5 SeitenHow Important Is It For COVID Vaccine Distribution To Be Given With Equal AccessJodi Bianca CerezoNoch keine Bewertungen
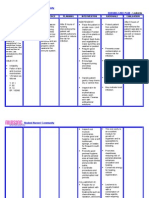
- Nursing Care Plan LeukemiaDokument2 SeitenNursing Care Plan Leukemiaderic87% (30)
- Hand InfectionsDokument30 SeitenHand Infectionsvinayguru82Noch keine Bewertungen
- Canine BabesiosisDokument10 SeitenCanine BabesiosisIonuț Gabriel ȚoleaNoch keine Bewertungen
- Blood TransfusionDokument2 SeitenBlood TransfusionAldwin Louis EstradaNoch keine Bewertungen
- Case MalariaDokument10 SeitenCase MalariasenioritaNoch keine Bewertungen
- Disease ArticleDokument29 SeitenDisease ArticleJozch EstebanNoch keine Bewertungen
- ENT Diseases of Paranasal SinusesDokument3 SeitenENT Diseases of Paranasal SinusesLucyellowOttemoesoeNoch keine Bewertungen
- Digging Up The Bones - MicrobiologyDokument31 SeitenDigging Up The Bones - MicrobiologyMossa Di Base100% (1)
- Organ TransplantationDokument36 SeitenOrgan TransplantationAnonymous 4TUSi0SqNoch keine Bewertungen
- CBC Interpetation Dr. MuslehDokument37 SeitenCBC Interpetation Dr. MuslehMusleh Al MusalhiNoch keine Bewertungen
- Widals TestDokument2 SeitenWidals TestEdgar DumagpiNoch keine Bewertungen
- Samples Received in 2014Dokument58 SeitenSamples Received in 2014Sameer KhanNoch keine Bewertungen
- Orbital CellulitisDokument21 SeitenOrbital CellulitisElsa Octavia100% (1)
- High Prevalence of KPC-2 Type Carbapenemase Coupled With CTX-M Type Extended-SpectrumDokument6 SeitenHigh Prevalence of KPC-2 Type Carbapenemase Coupled With CTX-M Type Extended-SpectrumMohammad K AlshomraniNoch keine Bewertungen
- Finals Biochemitry ReviewerDokument10 SeitenFinals Biochemitry Reviewerqwerty masterNoch keine Bewertungen
- Oie PDFDokument634 SeitenOie PDFFerdinand Prayogo Cahyo SantosoNoch keine Bewertungen
- MCQ On Immunity TypesDokument7 SeitenMCQ On Immunity Typessitalcoolk92% (12)
- Antiphospholipid Antibody SyndromeDokument273 SeitenAntiphospholipid Antibody SyndromeGeorgiana Murgu100% (2)
- Summary of Discussion About Skimming and ScanningDokument6 SeitenSummary of Discussion About Skimming and ScanningTri IndrawatiNoch keine Bewertungen
- NCMB 312 Lect Final NotesDokument16 SeitenNCMB 312 Lect Final NotesAngie BaylonNoch keine Bewertungen
- Pathophysiology of TBDokument3 SeitenPathophysiology of TBEddie Lou GuzmanNoch keine Bewertungen
- Non-Gonococcal Urethritis (NGU) : Signs and SymptomsDokument2 SeitenNon-Gonococcal Urethritis (NGU) : Signs and SymptomsIkhfa Yusril BahariNoch keine Bewertungen
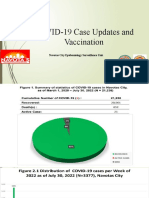
- Sdo Covid Monkey PoxDokument25 SeitenSdo Covid Monkey PoxRusty Lex FerrerNoch keine Bewertungen
- Balantidium ColiDokument12 SeitenBalantidium Colidaenil_oliverNoch keine Bewertungen
- Multiple MyelomaDokument5 SeitenMultiple Myelomaapi-647779956Noch keine Bewertungen
- Differential White Blood Cell CountDokument20 SeitenDifferential White Blood Cell CountNada hasan100% (2)
- Gambaran Penderita Infeksi Mata Di Rumah Sakit Mata Manado Provinsi Sulawesi Utara Periode Juni 2017 - Juni 2019Dokument5 SeitenGambaran Penderita Infeksi Mata Di Rumah Sakit Mata Manado Provinsi Sulawesi Utara Periode Juni 2017 - Juni 2019Darwin ThenNoch keine Bewertungen