Das könnte Ihnen auch gefallen
- Jurnal - A Comparative of Kojic Acid and Hydroquinone 2% Creams For The Treatment of Melasma PDFDokument5 SeitenJurnal - A Comparative of Kojic Acid and Hydroquinone 2% Creams For The Treatment of Melasma PDFHasepta Murfa YesiNoch keine Bewertungen
- Jurnal B 1Dokument10 SeitenJurnal B 1Nasayu Nadia Santika AyuNoch keine Bewertungen
- Jurnal Dr. FaisalDokument11 SeitenJurnal Dr. FaisalNasayu Nadia Santika AyuNoch keine Bewertungen
- Tenten TBMDokument2 SeitenTenten TBMNasayu Nadia Santika AyuNoch keine Bewertungen
- Jadwal Harian Baca SuratDokument1 SeiteJadwal Harian Baca SuratNasayu Nadia Santika AyuNoch keine Bewertungen
- Gawat Darurat Paru OK RevisedDokument121 SeitenGawat Darurat Paru OK RevisedNasayu Nadia Santika AyuNoch keine Bewertungen
- Gawat Darurat Paru OK RevisedDokument121 SeitenGawat Darurat Paru OK RevisedNasayu Nadia Santika AyuNoch keine Bewertungen
- Penyakit Saraf TepiDokument165 SeitenPenyakit Saraf TepiNasayu Nadia Santika AyuNoch keine Bewertungen
- BMI in PregnancyDokument4 SeitenBMI in PregnancyCitra KristiNoch keine Bewertungen
- Fenton2013growthchartcolor Girls PDFDokument1 SeiteFenton2013growthchartcolor Girls PDFNasayu Nadia Santika AyuNoch keine Bewertungen
- European Journal of Paediatric Neurology Volume Issue 2017 (Doi 10.1016/j.ejpn.2017.03.003) Wang, Shuai Wei, Yan-Zhao Yang, Jianhong Zhou, Yuming Zheng, - Clonidine Adhesive Patch For The TreatDokument27 SeitenEuropean Journal of Paediatric Neurology Volume Issue 2017 (Doi 10.1016/j.ejpn.2017.03.003) Wang, Shuai Wei, Yan-Zhao Yang, Jianhong Zhou, Yuming Zheng, - Clonidine Adhesive Patch For The TreatNasayu Nadia Santika AyuNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5784)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (72)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Tirotoxicosis Mayo Clinic Proceedings. Harma2019Dokument17 SeitenTirotoxicosis Mayo Clinic Proceedings. Harma2019Salome GarciaNoch keine Bewertungen
- Solution Manual For Mcgraw Hill Connect Resources For Jones Acquiring Medical Language 1eDokument58 SeitenSolution Manual For Mcgraw Hill Connect Resources For Jones Acquiring Medical Language 1ethomaslucasikwjeqyonm100% (29)
- Thyroid QuizDokument3 SeitenThyroid QuizĐặng Quỳnh ANNoch keine Bewertungen
- Thyroid Explain OsceDokument4 SeitenThyroid Explain OscerangaNoch keine Bewertungen
- Endocrinology 2015-2016 CM 377Dokument45 SeitenEndocrinology 2015-2016 CM 377Daniel ArseniNoch keine Bewertungen
- Primer: Graves' DiseaseDokument23 SeitenPrimer: Graves' DiseaseWidarsonNoch keine Bewertungen
- Management of Neonates Born To Mothers With Graves' Disease: BackgroundDokument13 SeitenManagement of Neonates Born To Mothers With Graves' Disease: BackgroundmariskaNoch keine Bewertungen
- Assessment of Serum Minerals and Electrolytes in TDokument5 SeitenAssessment of Serum Minerals and Electrolytes in THasni M MarsaolyNoch keine Bewertungen
- Thyroid DrugsDokument6 SeitenThyroid DrugsThe Real UploaderNoch keine Bewertungen
- IODINE - Solution To HealthproblemsDokument95 SeitenIODINE - Solution To Healthproblemshappycamper100% (59)
- Guideline For Hyperthyroidism ManagementDokument9 SeitenGuideline For Hyperthyroidism ManagementSyaimee Annisa AzzahraNoch keine Bewertungen
- Frequency Rate of Thyroid DiseaseDokument118 SeitenFrequency Rate of Thyroid DiseaseMustafa KhandgawiNoch keine Bewertungen
- Pituitary &thyroid NotesDokument7 SeitenPituitary &thyroid NotesAli salimNoch keine Bewertungen
- Pharmacology of The Endocrine SystemDokument74 SeitenPharmacology of The Endocrine SystemarpanabiswassshetyeNoch keine Bewertungen
- Medicine Long CaseDokument26 SeitenMedicine Long Casewhee182Noch keine Bewertungen
- HY Endocrine UsmleDokument22 SeitenHY Endocrine UsmleNakhal JararNoch keine Bewertungen
- "Oral Questions in Clinical Surgery" Case 1. LipomaDokument19 Seiten"Oral Questions in Clinical Surgery" Case 1. LipomaSherif Magdi100% (3)
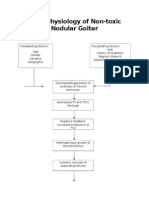
- Pathophysiology of Nontoxic Nodular GoiterDokument2 SeitenPathophysiology of Nontoxic Nodular GoiterJan Jewey80% (10)
- From The Division of Pharmacology, Hygienic Laboratory, Public Health and Marine Hospital Service, Washington, D. CDokument33 SeitenFrom The Division of Pharmacology, Hygienic Laboratory, Public Health and Marine Hospital Service, Washington, D. CAlexNoch keine Bewertungen
- Journal AnalysisDokument2 SeitenJournal AnalysisJust yor Regular CavegirlNoch keine Bewertungen
- "Nahadlok Naman Ko Sa Akong Gipambati, Ning-Undang Ko Sakong Work As QHSE and Training Manager, Nagdecide Ko Muuli Sa Pilipinas. Pag-Uli Nako Last Week, Ginabati Nako Mura Ko Makulbaan" AsDokument4 Seiten"Nahadlok Naman Ko Sa Akong Gipambati, Ning-Undang Ko Sakong Work As QHSE and Training Manager, Nagdecide Ko Muuli Sa Pilipinas. Pag-Uli Nako Last Week, Ginabati Nako Mura Ko Makulbaan" Ashanna caballoNoch keine Bewertungen
- Taylors.10 Minute - Diagnosis.manual - Symptoms.and - Signs.in - The.time Limited - Encounter.Dokument656 SeitenTaylors.10 Minute - Diagnosis.manual - Symptoms.and - Signs.in - The.time Limited - Encounter.micheal1960Noch keine Bewertungen
- High-Yield Endocrine Q&ADokument9 SeitenHigh-Yield Endocrine Q&ALillian Bezares100% (1)
- Thyroid and Antithyroid Drugs - PPTX - 20231126 - 103419 - 0000Dokument11 SeitenThyroid and Antithyroid Drugs - PPTX - 20231126 - 103419 - 0000Vaishnavi SheteNoch keine Bewertungen
- @MedicalBooksStore 2007 Self AssessmentDokument289 Seiten@MedicalBooksStore 2007 Self AssessmentOkka Soe OoNoch keine Bewertungen
- Med-Surg Final Exam Study GuideDokument3 SeitenMed-Surg Final Exam Study GuideLynn Suening100% (1)
- Drug Study (Tapazole)Dokument3 SeitenDrug Study (Tapazole)Izza DeloriaNoch keine Bewertungen
- GRP Specimenhandbook en 2004122807Dokument16 SeitenGRP Specimenhandbook en 2004122807AlibabarNoch keine Bewertungen
- Endocrine DisordersDokument77 SeitenEndocrine Disordersahmad100% (2)
- Surgical Pathology of the Thyroid GlandDokument15 SeitenSurgical Pathology of the Thyroid GlandAna CotomanNoch keine Bewertungen