Das könnte Ihnen auch gefallen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Lower Limb AnatomyDokument43 SeitenLower Limb AnatomyJason Toniolo100% (2)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Kegels For Men (Advanced PC Muscle Exercises) PDFDokument27 SeitenKegels For Men (Advanced PC Muscle Exercises) PDFSameer Joshi75% (4)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (894)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Clinical Cases in Physical Therapy 2nd Edition PDFDokument193 SeitenClinical Cases in Physical Therapy 2nd Edition PDFJohn Smith50% (2)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Urogenital PainDokument282 SeitenUrogenital PainAlex YoungNoch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
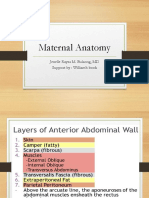
- Maternal Anatomy WilliamsDokument60 SeitenMaternal Anatomy WilliamsZari Novela100% (2)
- Counseling Theory SlidesDokument169 SeitenCounseling Theory Slidessanchu1981100% (3)
- OB MustKnowsDokument90 SeitenOB MustKnowsHarlyn MagsinoNoch keine Bewertungen
- PRI Integration For Geriatrics - Complete FileDokument159 SeitenPRI Integration For Geriatrics - Complete Filezhang yangNoch keine Bewertungen
- OB Williams Chap 2 Maternal AnatomyDokument7 SeitenOB Williams Chap 2 Maternal AnatomyRem Alfelor0% (1)
- Nursing ResearchDokument53 SeitenNursing ResearchFreeNursingNotes90% (21)
- How To Implement EcmDokument54 SeitenHow To Implement Ecmsanchu1981Noch keine Bewertungen
- 2 Abdominal and Pelvic AnatomyDokument47 Seiten2 Abdominal and Pelvic AnatomyNatalia VergaraNoch keine Bewertungen
- Uterovaginal ProlapseDokument52 SeitenUterovaginal ProlapseAmeera K Khan75% (4)
- IELTS Reading Answer SheetDokument1 SeiteIELTS Reading Answer Sheetskuppal50% (2)
- Clinical Cases in Physical Therapy 2nd EditionDokument193 SeitenClinical Cases in Physical Therapy 2nd Editionarghiralisa100% (21)
- Cgfns FormDokument29 SeitenCgfns Formapi-3712279100% (2)
- Old Is GoldDokument144 SeitenOld Is Goldnreena aslamNoch keine Bewertungen
- CH 2 - Maternal AnatomyDokument8 SeitenCH 2 - Maternal AnatomyRandom CommenterNoch keine Bewertungen
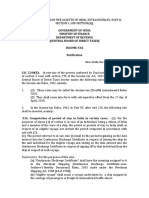
- Explanation: For The Purposes of This RuleDokument2 SeitenExplanation: For The Purposes of This Rulesanchu1981Noch keine Bewertungen
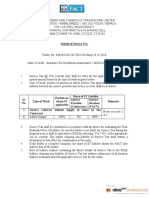
- Details of Service TaxDokument2 SeitenDetails of Service Taxsanchu1981Noch keine Bewertungen
- MDC BrochureDokument16 SeitenMDC Brochuresanchu1981Noch keine Bewertungen
- SPECIAL CONDITIONS CONTRACTDokument10 SeitenSPECIAL CONDITIONS CONTRACTsanchu1981Noch keine Bewertungen
- YCMOU-AST Syllabus T24 Diploma in Mechanical EngineeringDokument101 SeitenYCMOU-AST Syllabus T24 Diploma in Mechanical Engineeringsanchu1981Noch keine Bewertungen
- Signature Not Verified: Digitally Signed by SREEJITH B Date: 2016.10.24 16:38:05 IST Location: IndiaDokument1 SeiteSignature Not Verified: Digitally Signed by SREEJITH B Date: 2016.10.24 16:38:05 IST Location: Indiasanchu1981Noch keine Bewertungen
- Properties of Reinforcement PDFDokument6 SeitenProperties of Reinforcement PDFanmoljassalNoch keine Bewertungen
- Questions For CouncellingDokument3 SeitenQuestions For Councellingsanchu1981Noch keine Bewertungen
- I e Lts Writing Samples ADokument16 SeitenI e Lts Writing Samples Asanchu1981Noch keine Bewertungen
- Vapi CompaniesDokument9 SeitenVapi Companiessanchu19810% (1)
- IFE Qualifications and Relationship To National Occupational StandardsDokument6 SeitenIFE Qualifications and Relationship To National Occupational Standardssanchu1981Noch keine Bewertungen
- Compressed Air SystemDokument29 SeitenCompressed Air SystemPrathmesh GujaratiNoch keine Bewertungen
- CouncelingDokument34 SeitenCouncelingjahanbadsha100% (1)
- 2011 Research Outputs DefinitionsDokument39 Seiten2011 Research Outputs Definitionssanchu1981Noch keine Bewertungen
- Sail Trainee LD Apr Last ItiDokument6 SeitenSail Trainee LD Apr Last Itisanchu1981Noch keine Bewertungen
- Coal India Limited: CDSCRCDokument5 SeitenCoal India Limited: CDSCRCsanchu1981Noch keine Bewertungen
- Renewable NonrenewableDokument16 SeitenRenewable NonrenewableatulsemiloNoch keine Bewertungen
- US3857326Dokument6 SeitenUS3857326sanchu1981Noch keine Bewertungen
- Nursing Licensing Application Packet: WWW - Op.Nysed - GovDokument40 SeitenNursing Licensing Application Packet: WWW - Op.Nysed - Govsanchu1981Noch keine Bewertungen
- The New Generation of Bahco Socket SetsDokument8 SeitenThe New Generation of Bahco Socket Setssanchu1981Noch keine Bewertungen
- Maintenance and Welfare of Parents and Senior Citizens Act 2007Dokument7 SeitenMaintenance and Welfare of Parents and Senior Citizens Act 2007Kumar AshutoshNoch keine Bewertungen
- Rules, Regulations and Guidelines For Conducting Certificate Courses in The Faculty of Medicine and DentistryDokument8 SeitenRules, Regulations and Guidelines For Conducting Certificate Courses in The Faculty of Medicine and Dentistrysanchu1981Noch keine Bewertungen
- Chapter 12 Working DrawingDokument63 SeitenChapter 12 Working Drawingapi-200253170Noch keine Bewertungen
- Understanding Sports Hernia Athletic PubDokument40 SeitenUnderstanding Sports Hernia Athletic PubBichon OttawaNoch keine Bewertungen
- This Helix Trident Session Was A Dud I Broke A Couple of Rulesgqxsn PDFDokument18 SeitenThis Helix Trident Session Was A Dud I Broke A Couple of Rulesgqxsn PDFBabydolls27Noch keine Bewertungen
- Rectum and Anal CanalDokument44 SeitenRectum and Anal CanalAayush BhattaNoch keine Bewertungen
- Saraksha Orginal Thesis 2Dokument24 SeitenSaraksha Orginal Thesis 2Eashwar Prasad MeenakshiNoch keine Bewertungen
- Imperforate Anus and Cloacal MalformationsDokument23 SeitenImperforate Anus and Cloacal MalformationsGwyneth JangadNoch keine Bewertungen
- Pelvic Organ ProlapseDokument81 SeitenPelvic Organ ProlapseSasha VereeckenNoch keine Bewertungen
- Anatomy One Shot DR AshwiniDokument95 SeitenAnatomy One Shot DR Ashwinienthusiast383Noch keine Bewertungen
- 16 - Longer Stronger Orgasms For HimDokument26 Seiten16 - Longer Stronger Orgasms For HimEthan HillNoch keine Bewertungen
- Female External Genitalia AnatomyDokument3 SeitenFemale External Genitalia Anatomysharu4291Noch keine Bewertungen
- Board Review Axial Spine (Cervical, Thoracic, Lumbar, Sacrum, Pelvis, Cranial) Touro Burns 2022Dokument169 SeitenBoard Review Axial Spine (Cervical, Thoracic, Lumbar, Sacrum, Pelvis, Cranial) Touro Burns 2022Sean LeeNoch keine Bewertungen
- Prostate Fossa Contouring GuideDokument32 SeitenProstate Fossa Contouring GuideAna Paula IoostNoch keine Bewertungen
- Establishing a Peripartum Perineal Trauma ClinicDokument10 SeitenEstablishing a Peripartum Perineal Trauma ClinicmcastillomendozaNoch keine Bewertungen
- Pelvis and Perineum - ClinicalKeyDokument52 SeitenPelvis and Perineum - ClinicalKeyElianaNoch keine Bewertungen
- Clinical Anatomy of The Vulva, Vagina, Lower Pelvis, and PerineumDokument20 SeitenClinical Anatomy of The Vulva, Vagina, Lower Pelvis, and PerineumJacobMsangNoch keine Bewertungen
- Maternal AnatomyDokument27 SeitenMaternal AnatomyGio BalisiNoch keine Bewertungen
- Role of Homoeopathy in Haemorrhoids With Miasmatic ConceptsDokument26 SeitenRole of Homoeopathy in Haemorrhoids With Miasmatic ConceptsDr. Rajneesh Kumar Sharma MD Hom83% (6)
- 5 Pelvic Floor AJ 2022 v2Dokument79 Seiten5 Pelvic Floor AJ 2022 v2Husam OsmanNoch keine Bewertungen