Das könnte Ihnen auch gefallen
- Adult Health Nursing Phase I Thursday 6:00-9:00 PM: Irritable Bowel SyndromeDokument18 SeitenAdult Health Nursing Phase I Thursday 6:00-9:00 PM: Irritable Bowel SyndromeLavinia Malazarte CaballeroNoch keine Bewertungen
- Acute Liver Failure & Hepatorenal Syndrome Diagnosis and ManagementDokument53 SeitenAcute Liver Failure & Hepatorenal Syndrome Diagnosis and ManagementArnavjyoti DasNoch keine Bewertungen
- HepatitisDokument41 SeitenHepatitisAli Nawaz khanNoch keine Bewertungen
- Drug Induced Liver InjuryDokument13 SeitenDrug Induced Liver InjuryIhsan PutraNoch keine Bewertungen
- Acetaminophen Toxicity: Michira I Getange Umb/15-A/054Dokument31 SeitenAcetaminophen Toxicity: Michira I Getange Umb/15-A/054Ahmed Ben BellaNoch keine Bewertungen
- Acute Liver FailureDokument24 SeitenAcute Liver FailureMohd Johari Mohd ShafuwanNoch keine Bewertungen
- By DR.: Haitham Mokhtar Mohamed Abd AllahDokument101 SeitenBy DR.: Haitham Mokhtar Mohamed Abd AllahMohamed ElkadyNoch keine Bewertungen
- 2 Approach To Elevated LFTDokument59 Seiten2 Approach To Elevated LFTparik2321Noch keine Bewertungen
- Hepaticfailure 191217094905Dokument39 SeitenHepaticfailure 191217094905enam professorNoch keine Bewertungen
- Acute Liver FailureDokument69 SeitenAcute Liver FailureAsif.N.IqbalNoch keine Bewertungen
- Pharmacotherapy of Hepatic FailureDokument11 SeitenPharmacotherapy of Hepatic FailureMenna ElesawyNoch keine Bewertungen
- Acute HepatitisDokument36 SeitenAcute HepatitisMuhammad BilalNoch keine Bewertungen
- لقطة شاشة ٢٠٢٣-٠٢-١٩ في ٤.٠٢.١٥ مDokument62 Seitenلقطة شاشة ٢٠٢٣-٠٢-١٩ في ٤.٠٢.١٥ مMona YahyaNoch keine Bewertungen
- Approach To The Jaundiced Patient: Internal Medicine Survivor Series July 12, 2004 Joel Bruggen, MDDokument51 SeitenApproach To The Jaundiced Patient: Internal Medicine Survivor Series July 12, 2004 Joel Bruggen, MDYazeed SalemNoch keine Bewertungen
- Welcome To Journal Club Presentation: Presented byDokument54 SeitenWelcome To Journal Club Presentation: Presented byneptorNoch keine Bewertungen
- Hepatic Disease in PregnancyDokument37 SeitenHepatic Disease in PregnancyElisha Joshi100% (1)
- 3 and 4 Management of Medically CompromisedDokument63 Seiten3 and 4 Management of Medically Compromisedranareda499Noch keine Bewertungen
- (Lecture) Acute Liver FailureDokument60 Seiten(Lecture) Acute Liver FailureJirayu Puthhai100% (1)
- Acute Liver Failure Guide: Causes, Symptoms, Diagnosis & TreatmentDokument19 SeitenAcute Liver Failure Guide: Causes, Symptoms, Diagnosis & TreatmentAhmed AbdelkaderNoch keine Bewertungen
- Approach To Viral Hepatitis andDokument38 SeitenApproach To Viral Hepatitis andVijay ShankarNoch keine Bewertungen
- Liver LecDokument107 SeitenLiver LecNMD LIFESAVERNoch keine Bewertungen
- Liver TransplantationDokument17 SeitenLiver Transplantationa_m_elsheemy1931Noch keine Bewertungen
- Chapter - 2 - C - II Liver CirrhosisDokument39 SeitenChapter - 2 - C - II Liver CirrhosisEmmaNoch keine Bewertungen
- Presentation On Hepatic Failure: Presented By: Sandhya Harbola M.SC Nursing 1 Year PcnmsDokument54 SeitenPresentation On Hepatic Failure: Presented By: Sandhya Harbola M.SC Nursing 1 Year PcnmsShubham Singh BishtNoch keine Bewertungen
- Acute Liver FailureDokument57 SeitenAcute Liver FailureashokgswaminathanNoch keine Bewertungen
- Approach To The Patient With Liver DiseaseDokument75 SeitenApproach To The Patient With Liver Diseasegamal attamNoch keine Bewertungen
- Liver Cirrhosis LectureDokument83 SeitenLiver Cirrhosis LectureSheila Regina Tiza100% (1)
- Acute PancreatitisDokument60 SeitenAcute PancreatitisHara TsolakidouNoch keine Bewertungen
- Approach To: Liver Function Tests: Dr. Ashish October 11, 2019Dokument32 SeitenApproach To: Liver Function Tests: Dr. Ashish October 11, 2019Ashish SatyalNoch keine Bewertungen
- Fulminant Hepatic Failure: 7 October 2009 Morning Report Christine Williams, MDDokument25 SeitenFulminant Hepatic Failure: 7 October 2009 Morning Report Christine Williams, MDAndreas SichoneNoch keine Bewertungen
- Chapter 2 - C - III Portal HypertensionDokument37 SeitenChapter 2 - C - III Portal HypertensionEmmaNoch keine Bewertungen
- Acute PancreatitisDokument7 SeitenAcute PancreatitisVytheeshwaran Vedagiri100% (9)
- Irritable Bowel SyndromeDokument7 SeitenIrritable Bowel SyndromeLavinia Malazarte CaballeroNoch keine Bewertungen
- Acute Renal Failure: The Kidney Is Your Friend (Under 40 CharactersDokument31 SeitenAcute Renal Failure: The Kidney Is Your Friend (Under 40 CharactersAlina BoiangiuNoch keine Bewertungen
- Acutep 1Dokument45 SeitenAcutep 1api-19916399Noch keine Bewertungen
- Dr.P.santhosh Kumar Post GraduateDokument22 SeitenDr.P.santhosh Kumar Post GraduateSrilakshmi SathiyaNoch keine Bewertungen
- Anesthesia for Liver TransplantationDokument54 SeitenAnesthesia for Liver TransplantationPeeyoosh RaiNoch keine Bewertungen
- Stase Gastro SirosisDokument27 SeitenStase Gastro SirosisLuluFanDyNoch keine Bewertungen
- Acute Pancreatitis Signs, Causes, Diagnosis and TreatmentDokument21 SeitenAcute Pancreatitis Signs, Causes, Diagnosis and TreatmentRidwan kalibNoch keine Bewertungen
- Approach To The Patient With Abnormal Liver Tests: Alvaro Koch, M.DDokument47 SeitenApproach To The Patient With Abnormal Liver Tests: Alvaro Koch, M.DTimotius Kevin NatanaelNoch keine Bewertungen
- Presentation PDFDokument15 SeitenPresentation PDFعلا باسم عبد الكاظم جابر (تعليم موازي)Noch keine Bewertungen
- Pediatric Hepatitis - General PrinciplesDokument52 SeitenPediatric Hepatitis - General Principlesesra yulianaNoch keine Bewertungen
- Nafld: DR. Shatdal Chaudhary MDDokument42 SeitenNafld: DR. Shatdal Chaudhary MDWaqar AhmedNoch keine Bewertungen
- Anesthesia For Kidney DiseaseDokument6 SeitenAnesthesia For Kidney DiseaseFrits Dede SinagaNoch keine Bewertungen
- Hepatic Disorders: Prepared by Captain: Jumana AL-Momani RN - MSNDokument72 SeitenHepatic Disorders: Prepared by Captain: Jumana AL-Momani RN - MSNJanuaryNoch keine Bewertungen
- Hepatic Disorders Guide for CliniciansDokument42 SeitenHepatic Disorders Guide for CliniciansMimmey Yeniw100% (1)
- Drug-induced Liver Disease (DILD) Causes, Types, DiagnosisDokument30 SeitenDrug-induced Liver Disease (DILD) Causes, Types, DiagnosisSurya PratamaNoch keine Bewertungen
- Acute PancreatitisDokument40 SeitenAcute PancreatitisMustafa HusainNoch keine Bewertungen
- Anesthesia For Pts With Liver DiseaseDokument45 SeitenAnesthesia For Pts With Liver DiseaserijjorajooNoch keine Bewertungen
- Upper Gastrointestinal BleedingDokument49 SeitenUpper Gastrointestinal BleedingUmar AzlanNoch keine Bewertungen
- Feses IntroductionDokument88 SeitenFeses IntroductionAnisaPratiwiArumningsih100% (1)
- Interpretation of Liver Enzyme Tests - A Rapid GuideDokument3 SeitenInterpretation of Liver Enzyme Tests - A Rapid Guidesserggios100% (2)
- Acute Liver Failure-1Dokument40 SeitenAcute Liver Failure-1elizabethNoch keine Bewertungen
- Approach To The Jaundiced Patient: Internal Medicine Survivor Series July 12, 2004 Joel Bruggen, MDDokument51 SeitenApproach To The Jaundiced Patient: Internal Medicine Survivor Series July 12, 2004 Joel Bruggen, MDPutra SetiawanNoch keine Bewertungen
- AcuteHepatic Failure (Autosaved)Dokument32 SeitenAcuteHepatic Failure (Autosaved)Lakshmi prasad minnelaNoch keine Bewertungen
- Drug Induced Liver DisordersDokument31 SeitenDrug Induced Liver DisordersJason fernandes jNoch keine Bewertungen
- Acute and Chronic Liver Disease - Orla CrosbieDokument46 SeitenAcute and Chronic Liver Disease - Orla CrosbiewasimqureshiNoch keine Bewertungen
- Pathophysiology of Acute Liver FailureDokument39 SeitenPathophysiology of Acute Liver Failurelefebi6403Noch keine Bewertungen
- Agree ToolDokument59 SeitenAgree ToolCat NganNoch keine Bewertungen
- Ebcr Manu DraftDokument4 SeitenEbcr Manu DraftHeather PorterNoch keine Bewertungen
- QreqrqDokument1 SeiteQreqrqHeather PorterNoch keine Bewertungen
- Harald Seifert, Oliver Cornely, Kerstin Seggewiss, Mathias Decker, Danuta Stefanik, Hilmar Wisplinghoff, and Gerd Fa TkenheuerDokument6 SeitenHarald Seifert, Oliver Cornely, Kerstin Seggewiss, Mathias Decker, Danuta Stefanik, Hilmar Wisplinghoff, and Gerd Fa TkenheuerHeather PorterNoch keine Bewertungen
- TraumaDokument53 SeitenTraumaHeather PorterNoch keine Bewertungen
- GfsfsDokument30 SeitenGfsfsHeather PorterNoch keine Bewertungen
- Neutropenic Sepsis Prevention and 2 Management of Neutropenic Sepsis in 3 Cancer Patients PDFDokument242 SeitenNeutropenic Sepsis Prevention and 2 Management of Neutropenic Sepsis in 3 Cancer Patients PDFHeather PorterNoch keine Bewertungen
- Procalcitonin Guiding Antimicrobial PDFDokument4 SeitenProcalcitonin Guiding Antimicrobial PDFHeather PorterNoch keine Bewertungen
- Neutropenic Sepsis Prevention and 2 Management of Neutropenic Sepsis in 3 Cancer Patients PDFDokument242 SeitenNeutropenic Sepsis Prevention and 2 Management of Neutropenic Sepsis in 3 Cancer Patients PDFHeather PorterNoch keine Bewertungen
- Monitoring Procalcitonin in Febrile Neutropenia What Is PDFDokument9 SeitenMonitoring Procalcitonin in Febrile Neutropenia What Is PDFHeather PorterNoch keine Bewertungen
- PDFDokument14 SeitenPDFHeather PorterNoch keine Bewertungen
- Hyperemesis GravidarumDokument31 SeitenHyperemesis GravidarumFeregrine VerayoNoch keine Bewertungen
- Modern View of AsthmaDokument27 SeitenModern View of AsthmaraisaNoch keine Bewertungen
- Htnemergency 140524055705 Phpapp02Dokument75 SeitenHtnemergency 140524055705 Phpapp02Heather PorterNoch keine Bewertungen
- PRISMA-P Checklist for Systematic Review ProtocolDokument2 SeitenPRISMA-P Checklist for Systematic Review ProtocolHeather PorterNoch keine Bewertungen
- 2836 Full PDFDokument12 Seiten2836 Full PDFHeather PorterNoch keine Bewertungen
- Carcinoma of Unknown Primary Origin: Gauri R. VaradhacharyDokument7 SeitenCarcinoma of Unknown Primary Origin: Gauri R. VaradhacharyHeather PorterNoch keine Bewertungen
- Basic Chest X-Ray InterpretationDokument40 SeitenBasic Chest X-Ray InterpretationEzekiel Arteta0% (1)
- Aew 214Dokument11 SeitenAew 214Heather PorterNoch keine Bewertungen
- 1 Bridging Anticoag Primum Non NocereDokument12 Seiten1 Bridging Anticoag Primum Non NocereSpencerNoch keine Bewertungen
- Sle UpdateDokument5 SeitenSle UpdatePangeran AndiNoch keine Bewertungen
- Pleural Disease Chest DrainDokument7 SeitenPleural Disease Chest DrainAlina GheNoch keine Bewertungen
- Pleural Disease Chest DrainDokument7 SeitenPleural Disease Chest DrainAlina GheNoch keine Bewertungen
- BPHDokument33 SeitenBPHHeather PorterNoch keine Bewertungen
- Aew 214Dokument11 SeitenAew 214Heather PorterNoch keine Bewertungen
- Pemeriksaan PendengaranDokument63 SeitenPemeriksaan PendengaranHeather PorterNoch keine Bewertungen
- 2836 Full PDFDokument12 Seiten2836 Full PDFHeather PorterNoch keine Bewertungen
- Pendekatan Klinis Penurunan PendengaranDokument29 SeitenPendekatan Klinis Penurunan PendengaranHeather PorterNoch keine Bewertungen
- Audiologi DasarDokument21 SeitenAudiologi DasarHeather PorterNoch keine Bewertungen
- ToxicologyDokument15 SeitenToxicologySarah JaneNoch keine Bewertungen
- ParacetamolDokument24 SeitenParacetamolg20kp33% (3)
- Acetaminophen (Paracetamol) : Clinical ToxicologyDokument34 SeitenAcetaminophen (Paracetamol) : Clinical Toxicologymalak amerNoch keine Bewertungen
- Case Scenario No.11 Acetaminophen PoisoningDokument2 SeitenCase Scenario No.11 Acetaminophen PoisoningKiara Denise TamayoNoch keine Bewertungen
- Oral Paracetamol Prescribing Guideline Oct 2018 PDFDokument2 SeitenOral Paracetamol Prescribing Guideline Oct 2018 PDFBeby SartikaNoch keine Bewertungen
- Ibuprofen 150mg + Paracetamol 500mg (Combodex)Dokument15 SeitenIbuprofen 150mg + Paracetamol 500mg (Combodex)ddandan_2Noch keine Bewertungen
- Toxics: Pattern of Paracetamol Poisoning: Influence On Outcome and ComplicationsDokument11 SeitenToxics: Pattern of Paracetamol Poisoning: Influence On Outcome and Complicationsinfinity ooNoch keine Bewertungen
- Summary Product CharacDokument41 SeitenSummary Product CharacRani HadinataNoch keine Bewertungen
- Acute Paracetamol Poisoning Case Studies ReviewDokument5 SeitenAcute Paracetamol Poisoning Case Studies Reviewbiya ao0Noch keine Bewertungen
- Activated Charcoal in Resource Poor Settings Reviewing The EvidenceDokument5 SeitenActivated Charcoal in Resource Poor Settings Reviewing The EvidenceCarlos Laureano Martinez FloresNoch keine Bewertungen
- Leaflet Mucolator Acetylcysteine 200mg SachetsDokument2 SeitenLeaflet Mucolator Acetylcysteine 200mg Sachetsbakhtawar naseebNoch keine Bewertungen
- KGD 2 IvanDokument92 SeitenKGD 2 IvanrikarikaNoch keine Bewertungen
- Liver Case - Hepatic ToxicologyDokument2 SeitenLiver Case - Hepatic Toxicologysaya001Noch keine Bewertungen
- The Treatment and Management of Selfharm in Emergency Departments Slide Set Powerpoint 189897661Dokument41 SeitenThe Treatment and Management of Selfharm in Emergency Departments Slide Set Powerpoint 189897661Zorbey TurkalpNoch keine Bewertungen
- I. Common GI Presentations.: 1. The MouthDokument26 SeitenI. Common GI Presentations.: 1. The MouthFarah FarahNoch keine Bewertungen
- Acetaminophen (Paracetamol) Poisoning in Adults: Pathophysiology, Presentation, and Evaluation - UpToDateDokument21 SeitenAcetaminophen (Paracetamol) Poisoning in Adults: Pathophysiology, Presentation, and Evaluation - UpToDateSofi SuegosNoch keine Bewertungen
- Reading Sample Test 2 Question Paper Part A PDFDokument4 SeitenReading Sample Test 2 Question Paper Part A PDFRini ShijoyNoch keine Bewertungen
- Panadeine Faq PDFDokument7 SeitenPanadeine Faq PDFJohn GibbinsNoch keine Bewertungen
- APAP-McNeil Package-2002Dokument127 SeitenAPAP-McNeil Package-2002qiuy99Noch keine Bewertungen
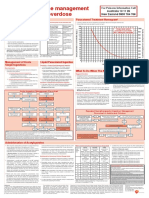
- Paracetamol OD Poster 2016 VersionDokument1 SeiteParacetamol OD Poster 2016 Versionmuhamed bwamkuuNoch keine Bewertungen
- Toxicology PDFDokument44 SeitenToxicology PDFhuong LNoch keine Bewertungen
- Acetaminophen Poisoning Case StudyDokument15 SeitenAcetaminophen Poisoning Case StudyseptianasptrNoch keine Bewertungen
- NurseLabs QnA#1Dokument41 SeitenNurseLabs QnA#1Jill NoelleNoch keine Bewertungen
- 1-Poisoning in Children Revised 2021Dokument63 Seiten1-Poisoning in Children Revised 2021Jawaher AbdullahNoch keine Bewertungen
- DNB Emergency Medicine Paper3Dokument5 SeitenDNB Emergency Medicine Paper3Vaishnavi AgrawalNoch keine Bewertungen
- Introduce The OTC Pain RelieversDokument9 SeitenIntroduce The OTC Pain RelieversNam's ThhanhNoch keine Bewertungen
- 01156Dokument13 Seiten01156riskysetNoch keine Bewertungen
- TOXICOLOGY MCQsDokument9 SeitenTOXICOLOGY MCQsSanjiv Sharma100% (1)
- Rokacet Rokacet PlusDokument11 SeitenRokacet Rokacet PlusNaomie bocobzaNoch keine Bewertungen
- 4 5820951304909882278 PDFDokument386 Seiten4 5820951304909882278 PDFMohamed HamoodNoch keine Bewertungen