Das könnte Ihnen auch gefallen
- SerratiopeptidaseDokument4 SeitenSerratiopeptidaseMo KhanNoch keine Bewertungen
- Benign Prostatic Hyperplasia PDFDokument496 SeitenBenign Prostatic Hyperplasia PDFnurul_nufafinaNoch keine Bewertungen
- Difficult Decisions in Colorectal PDFDokument578 SeitenDifficult Decisions in Colorectal PDFDenise Guevara100% (1)
- Red EyeDokument45 SeitenRed EyeDavidVictoriousLukas100% (1)
- Case Presentation 1Dokument27 SeitenCase Presentation 1Inatul Aulia67% (6)
- Comprehensive Health Care ServicesDokument18 SeitenComprehensive Health Care ServicesHamisu Tafashiya100% (1)
- Rhinology Fellowship InfoDokument2 SeitenRhinology Fellowship InfoSabyasachi Chakrabarti100% (3)
- Case Final THTDokument21 SeitenCase Final THTNadiah Baharum ShahNoch keine Bewertungen
- Parese Nervus III (Oculomotorius)Dokument26 SeitenParese Nervus III (Oculomotorius)jantyNoch keine Bewertungen
- ParkinsonDokument23 SeitenParkinsonHayley JuniorNoch keine Bewertungen
- TranslateDokument6 SeitenTranslatefsxxxxxNoch keine Bewertungen
- SMF Mata Rsud DR - Hi. Abdoel Moeloek Bandar LampungDokument6 SeitenSMF Mata Rsud DR - Hi. Abdoel Moeloek Bandar LampungNurulia AstriNoch keine Bewertungen
- Case Presentation 1 "OD Blepharoconjunctivitis Herpes Zoster Ophthalmica"Dokument37 SeitenCase Presentation 1 "OD Blepharoconjunctivitis Herpes Zoster Ophthalmica"Shirin LaleNoch keine Bewertungen
- Case ReportDokument23 SeitenCase ReportZacky Abdoel AzamNoch keine Bewertungen
- Ophtalmology Record Cataract: Examiner: Dr. Dr. Gilbert. W. Simanjuntak, SPM (K)Dokument6 SeitenOphtalmology Record Cataract: Examiner: Dr. Dr. Gilbert. W. Simanjuntak, SPM (K)NoviaNoch keine Bewertungen
- Status Ujian AfifDokument7 SeitenStatus Ujian AfifafifberlianNoch keine Bewertungen
- Traumatic Hyphema Os: Azillatin Ruhul Ma'Ani H1A014007Dokument20 SeitenTraumatic Hyphema Os: Azillatin Ruhul Ma'Ani H1A014007azillatinNoch keine Bewertungen
- CR Glaukoma Sek Ec UADokument12 SeitenCR Glaukoma Sek Ec UAtiffanyalmndNoch keine Bewertungen
- Case Report Glaukoma AkutDokument28 SeitenCase Report Glaukoma Akutnurul hidayahNoch keine Bewertungen
- Cataract Senilis Matur Od: Intania Rosati H1A013031 Supervisor: Dr. Siti Farida, SP.M (K)Dokument23 SeitenCataract Senilis Matur Od: Intania Rosati H1A013031 Supervisor: Dr. Siti Farida, SP.M (K)Intania RosatiNoch keine Bewertungen
- Ophtalmology RecordDokument8 SeitenOphtalmology RecordVebio RomatuaNoch keine Bewertungen
- CBD - DR Anna - DaraDokument10 SeitenCBD - DR Anna - DaraAulia Putri ANoch keine Bewertungen
- Case PersentationDokument28 SeitenCase PersentationAdisti NurutamiNoch keine Bewertungen
- Case PersentationDokument28 SeitenCase PersentationAdisti NurutamiNoch keine Bewertungen
- Ophtalmology Record ANGGA (ENG)Dokument7 SeitenOphtalmology Record ANGGA (ENG)alexxxxxNoch keine Bewertungen
- CBD - DR Anna SP - PD - Robby Gunawan - P21.1Dokument14 SeitenCBD - DR Anna SP - PD - Robby Gunawan - P21.1Robby GumawanNoch keine Bewertungen
- Status Kalazion - Yoga 1161050136Dokument10 SeitenStatus Kalazion - Yoga 1161050136Yoga WitularNoch keine Bewertungen
- Laporan Kasus Kelainan RefraksiDokument23 SeitenLaporan Kasus Kelainan RefraksiIchsan FajriNoch keine Bewertungen
- Status Kalazion - Yoga 1161050136Dokument10 SeitenStatus Kalazion - Yoga 1161050136Yoga WitularNoch keine Bewertungen
- Chapter IIIDokument6 SeitenChapter IIIPspduntanDuaribusebelasNoch keine Bewertungen
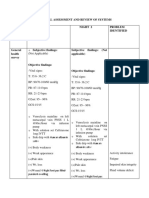
- Physical Assessment and Review of Systems Areas Assesse D Night 1 Night 2 Problem IdentifiedDokument9 SeitenPhysical Assessment and Review of Systems Areas Assesse D Night 1 Night 2 Problem IdentifiedAsniah Hadjiadatu AbdullahNoch keine Bewertungen
- Prista Examination OpthalmologyDokument7 SeitenPrista Examination OpthalmologyLamhotFarmaPurbaNoch keine Bewertungen
- Bab I Laporan Kasus: 1.1 Identitas PasienDokument6 SeitenBab I Laporan Kasus: 1.1 Identitas Pasienagung purmanaNoch keine Bewertungen
- MR 21 Maret 2022 Dr. YasaDokument26 SeitenMR 21 Maret 2022 Dr. YasaBaiq Bunga Citra PratiwiNoch keine Bewertungen
- Case Report WulanDokument11 SeitenCase Report Wulanwulan.yuniartiNoch keine Bewertungen
- Bab II AaDokument7 SeitenBab II AaPriskilaNoch keine Bewertungen
- General Anasthesia: Preceptor: Dr. H. Elya SP - AnDokument30 SeitenGeneral Anasthesia: Preceptor: Dr. H. Elya SP - AnMimin KurniaNoch keine Bewertungen
- CBD DR Anna SP - PD Robby Gunawan P21.1Dokument33 SeitenCBD DR Anna SP - PD Robby Gunawan P21.1Robby GumawanNoch keine Bewertungen
- Ophthalmology Record: Dr. Gilbert W. Simanjuntak, SP.M (K)Dokument6 SeitenOphthalmology Record: Dr. Gilbert W. Simanjuntak, SP.M (K)JackyHariantoNoch keine Bewertungen
- Pendarahan SubkonjungtivaDokument12 SeitenPendarahan SubkonjungtivaTyas AinunNoch keine Bewertungen
- 07 - 180 Diagnosis TBMDRDokument6 Seiten07 - 180 Diagnosis TBMDRlarasNoch keine Bewertungen
- Case Resume 19 Jan Edit 2Dokument33 SeitenCase Resume 19 Jan Edit 2Anangga AristantyoNoch keine Bewertungen
- Status Ujian Mata CitraDokument8 SeitenStatus Ujian Mata CitraFirda Diah UtamiNoch keine Bewertungen
- (Trauma) 06 - 07 - 2023 - SDR - Tantri - CKR 456 - Dr. Dana, SP.BDokument15 Seiten(Trauma) 06 - 07 - 2023 - SDR - Tantri - CKR 456 - Dr. Dana, SP.BRasyidu MashuriNoch keine Bewertungen
- Case Report KeratitisDokument6 SeitenCase Report KeratitisSeptianGunturNoch keine Bewertungen
- Cse reportTHTDokument12 SeitenCse reportTHTMichael Olivier WNoch keine Bewertungen
- Multiple Trauma Laporan KasusDokument13 SeitenMultiple Trauma Laporan KasusAnantaahNoch keine Bewertungen
- Case Based DiscussionDokument8 SeitenCase Based DiscussionNhinna Pinky'na BeibByNoch keine Bewertungen
- Final Perimembranous VSD CHDDokument28 SeitenFinal Perimembranous VSD CHDandayaannedhesireeNoch keine Bewertungen
- CBD - Dr. H. M. Saugi Abduh, SP - PD, KKV, Finasim - Laode Muhammad Sukarno K - CHFDokument38 SeitenCBD - Dr. H. M. Saugi Abduh, SP - PD, KKV, Finasim - Laode Muhammad Sukarno K - CHFkarnoNoch keine Bewertungen
- Morning Report Rsud Sayang RakyatDokument43 SeitenMorning Report Rsud Sayang RakyatRiski Wahyudi LasarikaNoch keine Bewertungen
- Keratitis: By: Eriska Ratnawati 18360196Dokument14 SeitenKeratitis: By: Eriska Ratnawati 18360196Diana Ulfah RahmanahNoch keine Bewertungen
- Emergency Department Report: Thursday, August 15, 2019 AYU / DIM / RAT/ YD.,MD.,Opthal. ConsultDokument27 SeitenEmergency Department Report: Thursday, August 15, 2019 AYU / DIM / RAT/ YD.,MD.,Opthal. ConsultdimasbudihartoNoch keine Bewertungen
- Miopi/Rabun Dekat: 1. DefinisiDokument3 SeitenMiopi/Rabun Dekat: 1. DefinisiIvan AlbertNoch keine Bewertungen
- Askep Pre Intra PostDokument43 SeitenAskep Pre Intra PostMuhammad Andhika PerkasaNoch keine Bewertungen
- Liskhairia - Spondilitis TuberculosaDokument25 SeitenLiskhairia - Spondilitis TuberculosaFiki FerindraNoch keine Bewertungen
- CBD Almira Salsabila - 30101507368 DR Saugi MAJUDokument160 SeitenCBD Almira Salsabila - 30101507368 DR Saugi MAJUJihan NabilaNoch keine Bewertungen
- Tutorial Dr. SaugiDokument33 SeitenTutorial Dr. SaugifemmytaniaNoch keine Bewertungen
- CBD DR Anna SP - PD - Neni Setyowati (30101700126)Dokument12 SeitenCBD DR Anna SP - PD - Neni Setyowati (30101700126)Neni SetyowatiNoch keine Bewertungen
- LAPORAN KASUS - Stroke IskemikDokument22 SeitenLAPORAN KASUS - Stroke IskemikMikhaNoch keine Bewertungen
- Ophtalmology Record Corneal Ulcer: Anggi Lewis R P Aruan 1161050113Dokument7 SeitenOphtalmology Record Corneal Ulcer: Anggi Lewis R P Aruan 1161050113LewishoppusNoch keine Bewertungen
- Status OftalmikusDokument2 SeitenStatus OftalmikusnicoNoch keine Bewertungen
- CBD Dr. Saugi - IstoyDokument41 SeitenCBD Dr. Saugi - IstoyAnonymous 6MjSEwhOgcNoch keine Bewertungen
- Audrey - Vertigo (Case Report) - DR Ronny Y SP SDokument24 SeitenAudrey - Vertigo (Case Report) - DR Ronny Y SP SaudreydesireeNoch keine Bewertungen
- Cataract Surgery Outcomes in Uveitis PDFDokument8 SeitenCataract Surgery Outcomes in Uveitis PDF-Yohanes Firmansyah-Noch keine Bewertungen
- LoA ISS Yana SylvanaDokument1 SeiteLoA ISS Yana Sylvana-Yohanes Firmansyah-Noch keine Bewertungen
- LoA ISS Hanna WijayaDokument1 SeiteLoA ISS Hanna Wijaya-Yohanes Firmansyah-Noch keine Bewertungen
- LoA ISS YohanesDokument1 SeiteLoA ISS Yohanes-Yohanes Firmansyah-Noch keine Bewertungen
- Presentation 1Dokument24 SeitenPresentation 1-Yohanes Firmansyah-Noch keine Bewertungen
- LoA ISS Michelle AngelikaDokument1 SeiteLoA ISS Michelle Angelika-Yohanes Firmansyah-Noch keine Bewertungen
- Anemia, Polycythemia, and White Blood Cell DisordersDokument22 SeitenAnemia, Polycythemia, and White Blood Cell Disorders-Yohanes Firmansyah-Noch keine Bewertungen
- Low Daily Dose of 3 MG Monacolin K From RYR Reduces The Concentration of LDLC in A Randomized Placebocontrolled InterventionDokument9 SeitenLow Daily Dose of 3 MG Monacolin K From RYR Reduces The Concentration of LDLC in A Randomized Placebocontrolled Intervention-Yohanes Firmansyah-Noch keine Bewertungen
- Clinical Characteristics and Visual Outcome of Severe Ocular Chemical Injuries in Shanghai PDFDokument5 SeitenClinical Characteristics and Visual Outcome of Severe Ocular Chemical Injuries in Shanghai PDF-Yohanes Firmansyah-Noch keine Bewertungen
- Weight-For-Age GIRLS: 6 Months To 2 Years (Z-Scores)Dokument1 SeiteWeight-For-Age GIRLS: 6 Months To 2 Years (Z-Scores)Malisa LukmanNoch keine Bewertungen
- EngDokument48 SeitenEngnina nurhayatiNoch keine Bewertungen
- Low Daily Dose of 3 MG Monacolin K From RYR Reduces The Concentration of LDLC in A Randomized Placebocontrolled InterventionDokument9 SeitenLow Daily Dose of 3 MG Monacolin K From RYR Reduces The Concentration of LDLC in A Randomized Placebocontrolled Intervention-Yohanes Firmansyah-Noch keine Bewertungen
- Cataract Surgery Outcomes in Uveitis The Multicenter Uveitis Steroid Treatment TrialDokument1 SeiteCataract Surgery Outcomes in Uveitis The Multicenter Uveitis Steroid Treatment Trial-Yohanes Firmansyah-Noch keine Bewertungen
- WHO - Haemoglobin Level For Anemia 2011Dokument6 SeitenWHO - Haemoglobin Level For Anemia 2011Adhi SanjayaNoch keine Bewertungen
- Gatifloxacin Versus Ceftriaxone For Uncomplicated Enteric Fever in Nepal An Openlabel Twocentre Randomised Controlled TrialDokument11 SeitenGatifloxacin Versus Ceftriaxone For Uncomplicated Enteric Fever in Nepal An Openlabel Twocentre Randomised Controlled Trial-Yohanes Firmansyah-Noch keine Bewertungen
- Wms GINA 2017 Main Report Tracked Changes For Archive PDFDokument156 SeitenWms GINA 2017 Main Report Tracked Changes For Archive PDFAnnisa MiendaNoch keine Bewertungen
- Fever PDFDokument6 SeitenFever PDF-Yohanes Firmansyah-Noch keine Bewertungen
- Effect of Amitriptyline and Escitalopram On Functional Dyspepsia A Multicenter Randomized Controlled Study-1Dokument12 SeitenEffect of Amitriptyline and Escitalopram On Functional Dyspepsia A Multicenter Randomized Controlled Study-1-Yohanes Firmansyah-Noch keine Bewertungen
- DyspepsiaDokument17 SeitenDyspepsia-Yohanes Firmansyah-Noch keine Bewertungen
- Metformin and Digestive DisordersDokument7 SeitenMetformin and Digestive Disorders-Yohanes Firmansyah-Noch keine Bewertungen
- Cause of Death in Patients With Diabetic CKD Enrolled in TheTrial To Reduce Cardiovascular Events With Aranesp TherapyTREATDokument12 SeitenCause of Death in Patients With Diabetic CKD Enrolled in TheTrial To Reduce Cardiovascular Events With Aranesp TherapyTREAT-Yohanes Firmansyah-Noch keine Bewertungen
- Glycemic Load Exercise and Monitoring Blood Glucose GEM A Paradigm Shift in The Treatment of Type 2 Diabetes MellitusDokument8 SeitenGlycemic Load Exercise and Monitoring Blood Glucose GEM A Paradigm Shift in The Treatment of Type 2 Diabetes Mellitus-Yohanes Firmansyah-Noch keine Bewertungen
- Efficacy of Nasal Mometasone For The Treatment of Chronic Sinonasal Disease in Patients With Inadequately Controlled AsthmaDokument14 SeitenEfficacy of Nasal Mometasone For The Treatment of Chronic Sinonasal Disease in Patients With Inadequately Controlled Asthma-Yohanes Firmansyah-Noch keine Bewertungen
- Antibiotik IDI Jakarta Utara 2015Dokument56 SeitenAntibiotik IDI Jakarta Utara 2015Natalia Devita SimorangkirNoch keine Bewertungen
- Efficacy of Transoral Fundoplication Vs Omeprazole For Treatment of Regurgitation in A Randomized Controlled Trial-1Dokument15 SeitenEfficacy of Transoral Fundoplication Vs Omeprazole For Treatment of Regurgitation in A Randomized Controlled Trial-1-Yohanes Firmansyah-Noch keine Bewertungen
- Glycemic Load Exercise and Monitoring Blood Glucose GEM A Paradigm Shift in The Treatment of Type 2 Diabetes MellitusDokument8 SeitenGlycemic Load Exercise and Monitoring Blood Glucose GEM A Paradigm Shift in The Treatment of Type 2 Diabetes Mellitus-Yohanes Firmansyah-Noch keine Bewertungen
- Cause of Death in Patients With Diabetic CKD Enrolled in TheTrial To Reduce Cardiovascular Events With Aranesp TherapyTREATDokument12 SeitenCause of Death in Patients With Diabetic CKD Enrolled in TheTrial To Reduce Cardiovascular Events With Aranesp TherapyTREAT-Yohanes Firmansyah-Noch keine Bewertungen
- Effect of Amitriptyline and Escitalopram On Functional Dyspepsia A Multicenter Randomized Controlled Study-1Dokument12 SeitenEffect of Amitriptyline and Escitalopram On Functional Dyspepsia A Multicenter Randomized Controlled Study-1-Yohanes Firmansyah-Noch keine Bewertungen
- Effect of Amitriptyline and Escitalopram On Functional Dyspepsia A Multicenter Randomized Controlled Study-1Dokument12 SeitenEffect of Amitriptyline and Escitalopram On Functional Dyspepsia A Multicenter Randomized Controlled Study-1-Yohanes Firmansyah-Noch keine Bewertungen
- Twenty Years of Progress On Maternal and Child Health in The Philippines: An Equity LensDokument10 SeitenTwenty Years of Progress On Maternal and Child Health in The Philippines: An Equity Lensnabila puti bachzaNoch keine Bewertungen
- Contagious Diseases in PHDokument10 SeitenContagious Diseases in PHJEnLipataNoch keine Bewertungen
- Poster-Youth Friendly SRH Services in SchoolsDokument1 SeitePoster-Youth Friendly SRH Services in SchoolsApril Rose Airoso - AramburoNoch keine Bewertungen
- Skin Rashes in ChildrenDokument11 SeitenSkin Rashes in ChildrenwiladamanikNoch keine Bewertungen
- Dermovate-NN Ointment: 1. What This Medicine Is and What It Is Used ForDokument1 SeiteDermovate-NN Ointment: 1. What This Medicine Is and What It Is Used ForIftikhar RasheedNoch keine Bewertungen
- Artikel No. 5 PCX - ReportDokument13 SeitenArtikel No. 5 PCX - ReportAnonymous Q6Ih0AfJNoch keine Bewertungen
- Simple Removable Appliances To Correct Anteriorand Posterior Crossbite in Mixed Dentition CaDokument9 SeitenSimple Removable Appliances To Correct Anteriorand Posterior Crossbite in Mixed Dentition Caadinda rachmaliaNoch keine Bewertungen
- Maxillary Canine-First Premolar TranspositionDokument9 SeitenMaxillary Canine-First Premolar TranspositionFabian BarretoNoch keine Bewertungen
- Health Information System SecondaryDokument6 SeitenHealth Information System SecondaryAlondra Aran0% (1)
- Ucsp 12 NAME: - GRADE and SECTION: - F. 7. C. Health As Human Right According To World Health Organization (WHO)Dokument1 SeiteUcsp 12 NAME: - GRADE and SECTION: - F. 7. C. Health As Human Right According To World Health Organization (WHO)Celia BautistaNoch keine Bewertungen
- Assessing The Ears and HearingDokument2 SeitenAssessing The Ears and HearingAL HAROUN ARAMAINNoch keine Bewertungen
- Introduction To PainDokument21 SeitenIntroduction To Painayanle Abdi AliNoch keine Bewertungen
- 1.1.2 OSH Foundations and Its Benefits - CEC 003-CEC32S6 - Construction Occupational Safety and Health (COSH)Dokument4 Seiten1.1.2 OSH Foundations and Its Benefits - CEC 003-CEC32S6 - Construction Occupational Safety and Health (COSH)RYAN JOSEPH QUIMONoch keine Bewertungen
- Acog Uso de Aspriian en El Embarazo PDFDokument15 SeitenAcog Uso de Aspriian en El Embarazo PDFAnghelino Jesus Meza CentenoNoch keine Bewertungen
- NCP HyperthermiaDokument2 SeitenNCP HyperthermiaKirby ContaoiNoch keine Bewertungen
- Occupational Health and Safety - 2Dokument4 SeitenOccupational Health and Safety - 2Kero KeropiNoch keine Bewertungen
- Maternal MidtermDokument253 SeitenMaternal MidtermTrishaNoch keine Bewertungen
- Nonpreemptive Goal Programing Method in Optimization Nurse Scheduling by Considering Education LevelDokument8 SeitenNonpreemptive Goal Programing Method in Optimization Nurse Scheduling by Considering Education LevelGabriel 15 MoseyNoch keine Bewertungen
- EthnolecrepooooorttpdfDokument61 SeitenEthnolecrepooooorttpdfNoelle Grace Ulep BaromanNoch keine Bewertungen
- Ac 76583 Pfdqwertaf 79898 TseDokument548 SeitenAc 76583 Pfdqwertaf 79898 TseMerve EmelNoch keine Bewertungen
- Treatment of Plaque-Induced Gingivitis Chronic PerDokument11 SeitenTreatment of Plaque-Induced Gingivitis Chronic PerAlleirbag KajnitisNoch keine Bewertungen
- Ahammer Halla Schneeweise JHE 2019Dokument20 SeitenAhammer Halla Schneeweise JHE 2019Grace HallaNoch keine Bewertungen
- PE and Health ReviewerDokument3 SeitenPE and Health ReviewerHat GuyNoch keine Bewertungen
- OB AssessmentDokument3 SeitenOB AssessmentJoshua D ParkerNoch keine Bewertungen