Das könnte Ihnen auch gefallen
- Composition and FunctionsDokument13 SeitenComposition and Functionsarun231187Noch keine Bewertungen
- ChromatographyDokument31 SeitenChromatographyarun231187Noch keine Bewertungen
- Specific Immune System: T - LymphocytesDokument18 SeitenSpecific Immune System: T - Lymphocytesarun231187Noch keine Bewertungen
- Effective Communication Between Physician and Pharmacist: Dr. G Praveen KumarDokument50 SeitenEffective Communication Between Physician and Pharmacist: Dr. G Praveen Kumararun231187Noch keine Bewertungen
- International University of Africa Faculty of Pharmacy Medicinal Chemistry MCHM 311 Siddieg Omer Elsiddieg, M. SC, B. SC (Honors)Dokument47 SeitenInternational University of Africa Faculty of Pharmacy Medicinal Chemistry MCHM 311 Siddieg Omer Elsiddieg, M. SC, B. SC (Honors)arun231187Noch keine Bewertungen
- Adsorption PresentationDokument23 SeitenAdsorption Presentationarun231187100% (1)
- Ureacycle ConversionDokument31 SeitenUreacycle Conversionarun231187Noch keine Bewertungen
- TwocomponentsystemDokument28 SeitenTwocomponentsystemarun231187Noch keine Bewertungen
- Unit 1 The Basis of BiochemistryDokument34 SeitenUnit 1 The Basis of Biochemistryarun231187Noch keine Bewertungen
- High Energy Compouds: Anjali.H.S BCH.10.05.10Dokument66 SeitenHigh Energy Compouds: Anjali.H.S BCH.10.05.10arun231187Noch keine Bewertungen
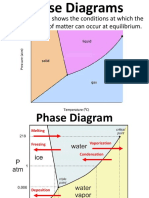
- A Phase Diagram Shows The Conditions at Which The Distinct Phases of Matter Can Occur at EquilibriumDokument9 SeitenA Phase Diagram Shows The Conditions at Which The Distinct Phases of Matter Can Occur at Equilibriumarun231187Noch keine Bewertungen
- Qualitativetestsforcarbohydrates 140615032421 Phpapp01Dokument52 SeitenQualitativetestsforcarbohydrates 140615032421 Phpapp01arun231187Noch keine Bewertungen
- PharmacologyDokument57 SeitenPharmacologyarun231187Noch keine Bewertungen
- Quality Control and Quality AssuranceDokument22 SeitenQuality Control and Quality Assurancearun231187Noch keine Bewertungen
- 06 Hinduismskybck 150217105249 Conversion Gate02Dokument142 Seiten06 Hinduismskybck 150217105249 Conversion Gate02arun231187Noch keine Bewertungen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Viral Markers Screening: King Khalid Hospital, NajranDokument1 SeiteViral Markers Screening: King Khalid Hospital, NajranCristal TannerNoch keine Bewertungen
- GCE 8807 Paper 1 (3) - GP May - June 2020Dokument4 SeitenGCE 8807 Paper 1 (3) - GP May - June 2020Menon HariNoch keine Bewertungen
- Syllabus - IM31202 - Statistical Learning With ApplicationsDokument3 SeitenSyllabus - IM31202 - Statistical Learning With Applicationsrohan kalidindiNoch keine Bewertungen
- Ch22 Managing A Holistic Marketing OrganizationDokument2 SeitenCh22 Managing A Holistic Marketing OrganizationRina Fordan Bilog100% (1)
- NCHRP RPT 568 - Riprap Design Criteria, Recommended Specifications and Quality ControlDokument226 SeitenNCHRP RPT 568 - Riprap Design Criteria, Recommended Specifications and Quality Controlaescarameia100% (1)
- BS7882 2008 Uncertainty Paper 2Dokument9 SeitenBS7882 2008 Uncertainty Paper 2Ian G. WalkerNoch keine Bewertungen
- RP 2009-10 Albert MwesigwaDokument70 SeitenRP 2009-10 Albert MwesigwaGeorge Baffour AwuahNoch keine Bewertungen
- Adversity QuotientDokument22 SeitenAdversity QuotientKimson JhunNoch keine Bewertungen
- Chapter - 3 Rev 2Dokument11 SeitenChapter - 3 Rev 2Merin sunilNoch keine Bewertungen
- Brainstorming For Research TopicsDokument18 SeitenBrainstorming For Research TopicsMa. Aiza SantosNoch keine Bewertungen
- Effects of Online Learning Mode in Psychological Aspect of College StudentsDokument4 SeitenEffects of Online Learning Mode in Psychological Aspect of College StudentsChrizel DiamanteNoch keine Bewertungen
- Rlverecio@lnu - Edu.ph Leyte Normal University, Tacloban City, PhilippinesDokument10 SeitenRlverecio@lnu - Edu.ph Leyte Normal University, Tacloban City, PhilippinesAnonymous PcPkRpAKD5Noch keine Bewertungen
- Veterinary Pharmacy, A Dismissed Necessity PDFDokument3 SeitenVeterinary Pharmacy, A Dismissed Necessity PDFKelma TayebaNoch keine Bewertungen
- Sandell - Social InclusionDokument18 SeitenSandell - Social InclusionFranciscoNoch keine Bewertungen
- VISA Processing AssistanceDokument1 SeiteVISA Processing AssistanceMC Alcazar ObedNoch keine Bewertungen
- Theory Based Evaluation: Past, Present, and FutureDokument19 SeitenTheory Based Evaluation: Past, Present, and FutureAlberto ComéNoch keine Bewertungen
- Internal Audit Sampling by IIADokument11 SeitenInternal Audit Sampling by IIAAndi Tri Jati86% (7)
- Marketing Intelligence & Planning: Article InformationDokument5 SeitenMarketing Intelligence & Planning: Article InformationAdrian SoareNoch keine Bewertungen
- Micro OB Syllabus - 18-20Dokument2 SeitenMicro OB Syllabus - 18-20Abhishek rajNoch keine Bewertungen
- N Sleeva Yamini Narisetty Mobile NoDokument3 SeitenN Sleeva Yamini Narisetty Mobile NoApoorva NarisettyNoch keine Bewertungen
- Carufel-Bye2020 Article ExplorationOfTheBodyGarmentRelDokument28 SeitenCarufel-Bye2020 Article ExplorationOfTheBodyGarmentRelAyşegül Yıldız KonukcuNoch keine Bewertungen
- Study Abroad Admission TimelineDokument4 SeitenStudy Abroad Admission TimelineAnupama PouloseNoch keine Bewertungen
- Willmott - Organization - Theory As Critical TheoryDokument42 SeitenWillmott - Organization - Theory As Critical Theoryekojulian_284861966Noch keine Bewertungen
- Frankel 1996Dokument16 SeitenFrankel 1996shaheerahmadNoch keine Bewertungen
- ChebyshevDokument3 SeitenChebyshevMajid Khammas NeamahNoch keine Bewertungen
- Handbook of Information 2017Dokument302 SeitenHandbook of Information 2017Shama ParveenNoch keine Bewertungen
- Generation X vs. Generation Y - A Decade of Online ShoppingDokument9 SeitenGeneration X vs. Generation Y - A Decade of Online ShoppingClaudiaNoch keine Bewertungen
- ENISA Cyber-Exercises Analysis Report-V1.0 PDFDokument32 SeitenENISA Cyber-Exercises Analysis Report-V1.0 PDFPaulo FelixNoch keine Bewertungen
- Artigo Publicado Revista Estudos de Psicologia Campinas 2022Dokument13 SeitenArtigo Publicado Revista Estudos de Psicologia Campinas 2022Antonio Augusto Pinto JuniorNoch keine Bewertungen
- Definition of Metropolitan Region in Various Countries: Definition by DickinsonDokument3 SeitenDefinition of Metropolitan Region in Various Countries: Definition by Dickinsonaditi kaviwalaNoch keine Bewertungen