Das könnte Ihnen auch gefallen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Kawasaki DiseaseDokument41 SeitenKawasaki DiseaseWuryan Dewi Mftahtyas ArumNoch keine Bewertungen
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Influenza 1918.0910Dokument19 SeitenInfluenza 1918.0910RafaelNoch keine Bewertungen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- Mayo Clinic BPPVDokument4 SeitenMayo Clinic BPPVCS NarayananNoch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Infections of The Eyes and The Central Nervous System by Dr. Joan E. CerradaDokument68 SeitenInfections of The Eyes and The Central Nervous System by Dr. Joan E. CerradaMonique BorresNoch keine Bewertungen
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- JaundiceDokument36 SeitenJaundiceNasser SalahNoch keine Bewertungen
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- COVID 19 Prevention Strategies for Healthcare WorkersDokument31 SeitenCOVID 19 Prevention Strategies for Healthcare WorkersPuteriNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Micro para The IntroductionDokument51 SeitenMicro para The IntroductionknotstmNoch keine Bewertungen
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Vaccines in Zimbabwe InformationDokument8 SeitenVaccines in Zimbabwe InformationIsaac GumboNoch keine Bewertungen
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- In-Hospital Cardiac Arrest A ReviewDokument11 SeitenIn-Hospital Cardiac Arrest A ReviewWawan JokoNoch keine Bewertungen
- Cudurrada CaruurtaDokument160 SeitenCudurrada CaruurtaHilowle YareNoch keine Bewertungen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- CANINE-Spontaneous Pneumothorax in DogsDokument7 SeitenCANINE-Spontaneous Pneumothorax in Dogstaner_soysurenNoch keine Bewertungen
- COPD Exacerbation Management Primary CareDokument1 SeiteCOPD Exacerbation Management Primary Caremufidah mawaddahNoch keine Bewertungen
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Types of Seizures: LIBAO, Kevin L. BSN-2HDokument3 SeitenTypes of Seizures: LIBAO, Kevin L. BSN-2HKevin100% (1)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Pengaruh Hipertensi Terhadap Kejadian Penyakit Jaringan Periodontal (Periodontitis) Pada Masyarakat Indonesia (Data Riskesdas 2018)Dokument8 SeitenPengaruh Hipertensi Terhadap Kejadian Penyakit Jaringan Periodontal (Periodontitis) Pada Masyarakat Indonesia (Data Riskesdas 2018)Brili AnenoNoch keine Bewertungen
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- 3rd Q LONG TEST IN HealthDokument2 Seiten3rd Q LONG TEST IN HealthDennmark IgutNoch keine Bewertungen
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- PSM Test Questions (5 Uni)Dokument14 SeitenPSM Test Questions (5 Uni)Phyo MaungNoch keine Bewertungen
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- COVID-19 Booster Eligibility All 3 BrandsDokument2 SeitenCOVID-19 Booster Eligibility All 3 BrandsJeff WattrickNoch keine Bewertungen
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- Tribute ofDokument10 SeitenTribute ofAlvaro Andres Flores JimenezNoch keine Bewertungen
- Dr. Rinrin Maharani's Curriculum Vitae and Initial Management for Acute StrokeDokument16 SeitenDr. Rinrin Maharani's Curriculum Vitae and Initial Management for Acute StrokeAyu WahyuniNoch keine Bewertungen
- NCM 111 RRL Chapter 2Dokument5 SeitenNCM 111 RRL Chapter 2kyle ibzNoch keine Bewertungen
- Gout and Pseudogout PDFDokument3 SeitenGout and Pseudogout PDFCarlNoch keine Bewertungen
- Frequency ListDokument386 SeitenFrequency ListParmar NileshNoch keine Bewertungen
- Uti Case Study (A.i)Dokument7 SeitenUti Case Study (A.i)Afkar IshakNoch keine Bewertungen
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- English SbaDokument21 SeitenEnglish Sbamickel cooperNoch keine Bewertungen
- TORCH in PregnancyDokument63 SeitenTORCH in PregnancyKinjal VasavaNoch keine Bewertungen
- Icicipru Smart Health LeafletDokument8 SeitenIcicipru Smart Health LeafletKuldip BarmanNoch keine Bewertungen
- Fungal InfectionsDokument8 SeitenFungal InfectionskateverdadNoch keine Bewertungen
- Lab Test Spot Urine Microalbumin Creatinine RatioDokument1 SeiteLab Test Spot Urine Microalbumin Creatinine Ratiorajanarora72Noch keine Bewertungen
- Jerome CornfieldDokument3 SeitenJerome CornfieldJohn Docherty100% (1)
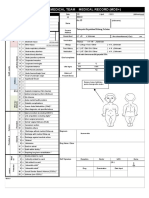
- Emergency Medical Team Medical Record (MDS+) : MDS - Check All That ApplyDokument2 SeitenEmergency Medical Team Medical Record (MDS+) : MDS - Check All That ApplySyafiraIdhatunNasyiahNoch keine Bewertungen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)