Das könnte Ihnen auch gefallen
- Kuliah Blok Growth and DevelopmentDokument44 SeitenKuliah Blok Growth and Developmentjaish8904Noch keine Bewertungen
- NICU Nutrition GuideDokument22 SeitenNICU Nutrition GuideStrept PneumoniaNoch keine Bewertungen
- Neonatal TPN: Dr. Fahad Al-AqlDokument10 SeitenNeonatal TPN: Dr. Fahad Al-AqlAnonymous 9dVZCnTXSNoch keine Bewertungen
- Parenteral Nutrition (PN) Clinical and Practical Considerations - CompressedDokument53 SeitenParenteral Nutrition (PN) Clinical and Practical Considerations - CompressedFiya AwanNoch keine Bewertungen
- Neonatal Parenteral Nutrition: Intensive Care Nursery House Staff ManualDokument7 SeitenNeonatal Parenteral Nutrition: Intensive Care Nursery House Staff ManualNugraha SultanNoch keine Bewertungen
- Principle of Pediatric Nutrition Care For ConsultantDokument17 SeitenPrinciple of Pediatric Nutrition Care For ConsultantvivydesyantiNoch keine Bewertungen
- Pediatric Nutritional AssessmentDokument51 SeitenPediatric Nutritional Assessmentcharanjit kaur100% (1)
- Medical Nutrition Therapy For Paediatric ConditionsDokument57 SeitenMedical Nutrition Therapy For Paediatric ConditionsﱞﱞﱞﱞﱞﱞﱞﱞﱞﱞﱞﱞﱞﱞﱞﱞﱞﱞﱞﱞﱞﱞﱞﱞNoch keine Bewertungen
- Nutrition Intervention - What's AvailableDokument39 SeitenNutrition Intervention - What's AvailablesitihawamtNoch keine Bewertungen
- Managing Diabetes Through Proper Treatment and MonitoringDokument10 SeitenManaging Diabetes Through Proper Treatment and Monitoringjoeln_9Noch keine Bewertungen
- Drug-Nutrient Interaction in Prescriptions ForDokument7 SeitenDrug-Nutrient Interaction in Prescriptions ForRafika DitaNoch keine Bewertungen
- Nutritional AssessmentDokument7 SeitenNutritional AssessmentSaher YasinNoch keine Bewertungen
- Session 2 Basics of NutritionDokument39 SeitenSession 2 Basics of NutritionAllyeah bethel GrupoNoch keine Bewertungen
- Nutrition Care Process Note-IcuDokument2 SeitenNutrition Care Process Note-Icuapi-1032325430% (1)
- Severe Acute Malnutrition and Fluid Management inDokument76 SeitenSevere Acute Malnutrition and Fluid Management inBibsNoch keine Bewertungen
- Nutrition - TPN (Basics)Dokument37 SeitenNutrition - TPN (Basics)Giorgi BradNoch keine Bewertungen
- 24 HR Food RecallDokument39 Seiten24 HR Food RecallKon Zhen JieNoch keine Bewertungen
- 406 ReflectionDokument1 Seite406 Reflectionapi-533641139Noch keine Bewertungen
- Parenteral Nutrition: Indications and RequirementsDokument56 SeitenParenteral Nutrition: Indications and RequirementsdenekeNoch keine Bewertungen
- Operational Guidelines Acute Malnutrition South Africa FINAL-1!8!15-2Dokument70 SeitenOperational Guidelines Acute Malnutrition South Africa FINAL-1!8!15-2RajabSaputra100% (2)
- Nutritional Disorders in Filipino ChildrenDokument9 SeitenNutritional Disorders in Filipino ChildrenJill Sanchez-SadiaNoch keine Bewertungen
- Medicine and Nutrition Case StudyDokument5 SeitenMedicine and Nutrition Case Studyapi-384113918Noch keine Bewertungen
- Nutrition PaperDokument4 SeitenNutrition Paperapi-433705780Noch keine Bewertungen
- Health Assessment AssignmentDokument8 SeitenHealth Assessment Assignmentapi-314827222100% (1)
- Nutrition Management Premie NashDokument49 SeitenNutrition Management Premie NashathaNoch keine Bewertungen
- Vitamin B12 Deficiency and A Patient Case StudyDokument36 SeitenVitamin B12 Deficiency and A Patient Case Studynherm6425100% (1)
- PES StatementsDokument6 SeitenPES Statementsdoniazad13112Noch keine Bewertungen
- Unani Medicine for IBSDokument26 SeitenUnani Medicine for IBSDr. Md. Shahab UddinNoch keine Bewertungen
- PN Monitoring and ComplicationsDokument35 SeitenPN Monitoring and ComplicationsRhomizal Mazali100% (1)
- Nutrition Care Process WorksheetDokument7 SeitenNutrition Care Process Worksheetapi-338119904Noch keine Bewertungen
- Complementary FeedingDokument38 SeitenComplementary FeedingsitihawamtNoch keine Bewertungen
- Diet TherapyDokument140 SeitenDiet Therapyraghadalesawi51Noch keine Bewertungen
- Nutritional DisordersDokument50 SeitenNutritional Disorderstayyab khanNoch keine Bewertungen
- Medical Nutrition Therapy For DiabetesDokument27 SeitenMedical Nutrition Therapy For DiabetesAlfitri YuniNoch keine Bewertungen
- Dietary Intake AssessmentDokument4 SeitenDietary Intake AssessmentMary Mae BuellaNoch keine Bewertungen
- Nutritional Issues in The ICU Case FileDokument2 SeitenNutritional Issues in The ICU Case Filehttps://medical-phd.blogspot.com100% (1)
- Nutrition During LactationDokument25 SeitenNutrition During LactationDaniel HeryantoNoch keine Bewertungen
- Hospital DietsDokument1 SeiteHospital DietsAnne Julia AgustinNoch keine Bewertungen
- Nutrition: - . - and The Surgical Patient (Pre and Post Operative Nutrition)Dokument58 SeitenNutrition: - . - and The Surgical Patient (Pre and Post Operative Nutrition)SanaSofiyahNoch keine Bewertungen
- Essential Enteral and Parenteral Nutrition GuideDokument64 SeitenEssential Enteral and Parenteral Nutrition GuideHeba IyadNoch keine Bewertungen
- The Registered Dietitian: Perceptions, Assumptions, and RealityDokument50 SeitenThe Registered Dietitian: Perceptions, Assumptions, and RealityARKressNoch keine Bewertungen
- Nutrition in ICU: DR Rahul VarshenyDokument50 SeitenNutrition in ICU: DR Rahul VarshenyAntar InenigogNoch keine Bewertungen
- MNT for Diabetes Nutrition TherapyDokument27 SeitenMNT for Diabetes Nutrition Therapydr.Uci BaharNoch keine Bewertungen
- Public Health NutritionDokument58 SeitenPublic Health NutritionJaime TaylorNoch keine Bewertungen
- Pes Statements SamplesDokument19 SeitenPes Statements SamplesJennie ManobanNoch keine Bewertungen
- Case Study 19Dokument3 SeitenCase Study 19api-533641139Noch keine Bewertungen
- Nutr 510 - Counseling Session 2Dokument4 SeitenNutr 510 - Counseling Session 2api-240740872Noch keine Bewertungen
- Low Birthweight InfantDokument42 SeitenLow Birthweight InfantJoNoch keine Bewertungen
- 12 Neonatal Hypocalcemia, Glycemia and MagnesemiaDokument55 Seiten12 Neonatal Hypocalcemia, Glycemia and MagnesemiaRana Vandana100% (1)
- Energy Intake and ExpenditureDokument38 SeitenEnergy Intake and ExpenditureNichNoch keine Bewertungen
- Protocal Followed For Enteral FeedingDokument4 SeitenProtocal Followed For Enteral FeedingK Jayakumar KandasamyNoch keine Bewertungen
- Katherine Orourke Resume With ReferencesDokument2 SeitenKatherine Orourke Resume With Referencesapi-485480196Noch keine Bewertungen
- Nurses' Role in Nutrition and DieteticsDokument53 SeitenNurses' Role in Nutrition and DieteticsLouie ParillaNoch keine Bewertungen
- Enteral Nutrition Manual Oct 2011Dokument51 SeitenEnteral Nutrition Manual Oct 2011Salilah Mahfudz100% (1)
- Total Parenteral Nutrition:: By: Group 4Dokument25 SeitenTotal Parenteral Nutrition:: By: Group 4Mylz MendozaNoch keine Bewertungen
- Safe Upper Levels For Vitamins and Minerals (FSA)Dokument360 SeitenSafe Upper Levels For Vitamins and Minerals (FSA)jcpchin2Noch keine Bewertungen
- Gastrointestinal Diseases and Disorders Sourcebook, Fifth EditionVon EverandGastrointestinal Diseases and Disorders Sourcebook, Fifth EditionNoch keine Bewertungen
- Guidelines for Measuring Household and Individual Dietary DiversityVon EverandGuidelines for Measuring Household and Individual Dietary DiversityNoch keine Bewertungen
- Obstetrics Study Guide on Hypertension, Preterm Labor, InfectionDokument172 SeitenObstetrics Study Guide on Hypertension, Preterm Labor, InfectionAnonymous N2PHMnTIYLNoch keine Bewertungen
- PPROMDokument55 SeitenPPROMAnonymous N2PHMnTIYLNoch keine Bewertungen
- FertilisasiDokument18 SeitenFertilisasiAnonymous N2PHMnTIYLNoch keine Bewertungen
- Kuliah Blok 2 Gangguan Hemodinamik Trombosis Dan ShockDokument37 SeitenKuliah Blok 2 Gangguan Hemodinamik Trombosis Dan ShockAnonymous N2PHMnTIYLNoch keine Bewertungen
- What Did You Learn Tuday Dear Indira Cari PentingDokument1 SeiteWhat Did You Learn Tuday Dear Indira Cari PentingAnonymous N2PHMnTIYLNoch keine Bewertungen
- Curriculum Vitae: Personal IdentificationDokument2 SeitenCurriculum Vitae: Personal IdentificationAnonymous N2PHMnTIYLNoch keine Bewertungen
- Belajar Bahasa InggrisDokument2 SeitenBelajar Bahasa InggrisAnonymous N2PHMnTIYLNoch keine Bewertungen
- What Did You Learn Tuday Dear Indira Cari PentingDokument1 SeiteWhat Did You Learn Tuday Dear Indira Cari PentingAnonymous N2PHMnTIYLNoch keine Bewertungen
- Banana - Recommendations For Maintaining Postharvest Quality - Postharvest Technology Center - UC Davis PDFDokument3 SeitenBanana - Recommendations For Maintaining Postharvest Quality - Postharvest Technology Center - UC Davis PDFFernando SanchezNoch keine Bewertungen
- FOI Research On AcupunctureDokument118 SeitenFOI Research On AcupunctureDilutionsUKNoch keine Bewertungen
- Proliferation Therapy for Tendon and Ligament InjuriesDokument18 SeitenProliferation Therapy for Tendon and Ligament InjuriesJason Tutt GinNoch keine Bewertungen
- Department Check List Final 3Dokument27 SeitenDepartment Check List Final 3BOOKREADER_NOWNoch keine Bewertungen
- FMST 314 Finals NotesDokument8 SeitenFMST 314 Finals NotesmoomoomaoNoch keine Bewertungen
- Parkinson DiseaseDokument9 SeitenParkinson DiseaseMarco GunawanNoch keine Bewertungen
- IHI Global Trigger ToolDokument46 SeitenIHI Global Trigger ToolJuan Manuel LujanNoch keine Bewertungen
- Narrative TherapyDokument11 SeitenNarrative TherapyCamila Orellana100% (1)
- Ot ProtocolDokument38 SeitenOt ProtocolSelva KumarNoch keine Bewertungen
- Categories of Disability Under IDEADokument6 SeitenCategories of Disability Under IDEANational Dissemination Center for Children with DisabilitiesNoch keine Bewertungen
- CTCAE 4.03 2010-06-14 QuickReference 5x7Dokument196 SeitenCTCAE 4.03 2010-06-14 QuickReference 5x7Andreea ZaharieNoch keine Bewertungen
- Treatment of Pregnancy-Related Lumbar and Pelvic Girdle Pain by The Yoga Method: A Randomized Controlled StudyDokument8 SeitenTreatment of Pregnancy-Related Lumbar and Pelvic Girdle Pain by The Yoga Method: A Randomized Controlled StudyJosephineeNoch keine Bewertungen
- Fred Maiorino CaseDokument11 SeitenFred Maiorino CaseGajo VankaNoch keine Bewertungen
- Chapter 4 - P4 P5 The Role of Complementary TherapiesDokument8 SeitenChapter 4 - P4 P5 The Role of Complementary TherapiesdesbestNoch keine Bewertungen
- 7th Panhellenic Congress of Thermal MedicineDokument6 Seiten7th Panhellenic Congress of Thermal MedicineEmmanuel Manolis KosadinosNoch keine Bewertungen
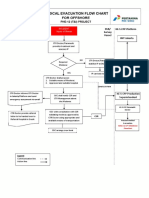
- 3-A4 - Medical Evacuation Flow Chart (Rev.0)Dokument1 Seite3-A4 - Medical Evacuation Flow Chart (Rev.0)SiskaNoch keine Bewertungen
- HeelDokument4 SeitenHeelDoha EbedNoch keine Bewertungen
- Platelet-Rich Plasma For Hair Restoration: Natalie Justicz,, Adeeb Derakhshan,, Jenny X. Chen,, Linda N. LeeDokument7 SeitenPlatelet-Rich Plasma For Hair Restoration: Natalie Justicz,, Adeeb Derakhshan,, Jenny X. Chen,, Linda N. Leejaviers45Noch keine Bewertungen
- ArdsDokument29 SeitenArdsAmani KayedNoch keine Bewertungen
- Water Supply and Sanitary Engineering by Chittaranjan Bibhar 2cfa37 PDFDokument115 SeitenWater Supply and Sanitary Engineering by Chittaranjan Bibhar 2cfa37 PDFRahul TomarNoch keine Bewertungen
- Final Submission UpdatedDokument26 SeitenFinal Submission Updatedapi-528981305Noch keine Bewertungen
- Antenatal CareDokument4 SeitenAntenatal Caredrfaruqui2551100% (1)
- Adrenal Care ShaktiDokument12 SeitenAdrenal Care ShaktiAnonymous 7R6n0f9BY100% (2)
- Case Presentation BronchiectasisDokument61 SeitenCase Presentation BronchiectasisUzair Muhd100% (6)
- Tress Test: The Gale Encyclopedia of MedicineDokument7 SeitenTress Test: The Gale Encyclopedia of MedicineSalsabilla KimikoNoch keine Bewertungen
- Neonatal Resuscitation Power PointDokument29 SeitenNeonatal Resuscitation Power PointsameerarswNoch keine Bewertungen
- Intramuscular CKLDokument2 SeitenIntramuscular CKLapi-310181843Noch keine Bewertungen
- Quinine 1Dokument3 SeitenQuinine 1Vhan BetizNoch keine Bewertungen
- PsychopathiaDokument26 SeitenPsychopathiaKunal KejriwalNoch keine Bewertungen
- Test Bank For Maternal Child Nursing 5th EditionDokument8 SeitenTest Bank For Maternal Child Nursing 5th EditionJennifer Burke100% (34)