Das könnte Ihnen auch gefallen
- ALU 201 Practice QuestionsDokument15 SeitenALU 201 Practice QuestionsPeter100% (1)
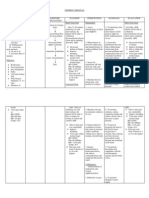
- NURSING CARE PLAN For Myocardial InfarctionDokument13 SeitenNURSING CARE PLAN For Myocardial Infarctionbanyenye2593% (14)
- Cardiac Function TestDokument8 SeitenCardiac Function Testramanrajesh83100% (2)
- Acute Coronary Syndrome - A Case StudyDokument11 SeitenAcute Coronary Syndrome - A Case StudyRocel Devilles100% (2)
- Compartment SyndromeDokument23 SeitenCompartment SyndromeTufikifa N. NakaleNoch keine Bewertungen
- Stroke PathophysiologyDokument3 SeitenStroke PathophysiologyMaureen Balagtas89% (9)
- AtherosclerosisDokument56 SeitenAtherosclerosisJohn Matley Caampued100% (8)
- Surgical Coronary Revascularization Who, What, WhenDokument68 SeitenSurgical Coronary Revascularization Who, What, WhenAlaaGaballaNoch keine Bewertungen
- ESC-2023 Day 3 UpdatesDokument41 SeitenESC-2023 Day 3 UpdatesIvan TeongNoch keine Bewertungen
- Preoperative Cardiac Risk Assessment in Noncardiac SurgeryDokument13 SeitenPreoperative Cardiac Risk Assessment in Noncardiac SurgeryOgbonnaya IfeanyichukwuNoch keine Bewertungen
- Cardiovascular DiseaseDokument12 SeitenCardiovascular DiseaseVipul NagnesiaNoch keine Bewertungen
- Heart Transplant ContentDokument17 SeitenHeart Transplant ContentrajNoch keine Bewertungen
- Ischemic Heart Disease Anaesthetic Management For Elective and Emergency SurgeriesDokument57 SeitenIschemic Heart Disease Anaesthetic Management For Elective and Emergency SurgeriesCutie PieNoch keine Bewertungen
- Preoperative Management of Patients Undergoing AnaesthesiaDokument24 SeitenPreoperative Management of Patients Undergoing AnaesthesiaGx NavinNoch keine Bewertungen
- 3 NopalpamogasDokument5 Seiten3 NopalpamogasFeb NamiaNoch keine Bewertungen
- Cmas 101 BJDokument4 SeitenCmas 101 BJSurya BhupatirajuNoch keine Bewertungen
- Arritmias Ventriculares en Paciente Con Cardiomiopatia No IsquemicaDokument2 SeitenArritmias Ventriculares en Paciente Con Cardiomiopatia No Isquemicatere glezNoch keine Bewertungen
- Surgical Intervention in Management of Heart Failure: DR Royman Simanjuntak Sp. BTKVDokument118 SeitenSurgical Intervention in Management of Heart Failure: DR Royman Simanjuntak Sp. BTKVEmily RumiaNoch keine Bewertungen
- Preoperative Cardiac Risk Assessment in Noncardiac SurgeryDokument6 SeitenPreoperative Cardiac Risk Assessment in Noncardiac SurgeryOgbonnaya IfeanyichukwuNoch keine Bewertungen
- RANASINGHE Cardiac Function & Disease & AnesthesiaDokument51 SeitenRANASINGHE Cardiac Function & Disease & AnesthesiaDagimNoch keine Bewertungen
- Preoreoperative Cardiac AssessmentDokument71 SeitenPreoreoperative Cardiac AssessmentHossam atefNoch keine Bewertungen
- Geron CardioDokument45 SeitenGeron CardioApril AlomiaNoch keine Bewertungen
- Insuficienta Cardiaca PerioperatorieDokument123 SeitenInsuficienta Cardiaca Perioperatoriemd.dascalescu2486Noch keine Bewertungen
- Cardiac Periop ManagementDokument96 SeitenCardiac Periop ManagementCorina FoiaNoch keine Bewertungen
- Perioperative Cardiovascular Evaluation DR Gage 3-22-2004Dokument20 SeitenPerioperative Cardiovascular Evaluation DR Gage 3-22-2004anu1101Noch keine Bewertungen
- Cardiac ResuscitationDokument24 SeitenCardiac ResuscitationPaulinaNoch keine Bewertungen
- Marie M Altenburg Diagnosis and Management of AorticDokument2 SeitenMarie M Altenburg Diagnosis and Management of AorticAnanth BalakrishnanNoch keine Bewertungen
- Edited Cardiovascular Evaluation in Patients Undergo Non-Cardiac Surgery - Gadis Virza - Dr. Nur HaryonoDokument26 SeitenEdited Cardiovascular Evaluation in Patients Undergo Non-Cardiac Surgery - Gadis Virza - Dr. Nur HaryonoFikriYTNoch keine Bewertungen
- Non Cardiac OpDokument21 SeitenNon Cardiac Opc4ri5Noch keine Bewertungen
- TOPIC1Chronic Forms of Coronary Heart DiseaseDokument3 SeitenTOPIC1Chronic Forms of Coronary Heart DiseaseAdi PomeranzNoch keine Bewertungen
- Ucm 497098 PDFDokument103 SeitenUcm 497098 PDFJusma Wijaya Kusuma GNoch keine Bewertungen
- ACHD ACC GuidelinesDokument91 SeitenACHD ACC Guidelinessamir poudelNoch keine Bewertungen
- Review Articles: Medical ProgressDokument10 SeitenReview Articles: Medical ProgressMiko AkmarozaNoch keine Bewertungen
- Essential Messages - 2023 ACSDokument16 SeitenEssential Messages - 2023 ACSimran karimNoch keine Bewertungen
- Overview of Exercise Stress Testing: Suleiman M Kharabsheh, Abdulaziz Al-Sugair, Jehad Al-Buraiki, Joman FarhanDokument6 SeitenOverview of Exercise Stress Testing: Suleiman M Kharabsheh, Abdulaziz Al-Sugair, Jehad Al-Buraiki, Joman FarhanDicky PayungNoch keine Bewertungen
- Overview of Exercise Stress Testing: Suleiman M Kharabsheh, Abdulaziz Al-Sugair, Jehad Al-Buraiki, Joman FarhanDokument6 SeitenOverview of Exercise Stress Testing: Suleiman M Kharabsheh, Abdulaziz Al-Sugair, Jehad Al-Buraiki, Joman FarhanMilan AnandNoch keine Bewertungen
- CardiologyDokument102 SeitenCardiologyashrafholailNoch keine Bewertungen
- Cardiac SurgeryDokument19 SeitenCardiac SurgerySimon JosanNoch keine Bewertungen
- Anaesthetic Implications in A Patient With Poor LV Function by DR Sanjula VirmaniDokument39 SeitenAnaesthetic Implications in A Patient With Poor LV Function by DR Sanjula VirmanicardiacanesthesiaNoch keine Bewertungen
- A Report of The American College of Cardiology/American Heart Association Task Force On Practice GuidelinesDokument47 SeitenA Report of The American College of Cardiology/American Heart Association Task Force On Practice GuidelinesAsawin RungpattanakijchaiNoch keine Bewertungen
- View Topic Percutaneous Coronary Intervention Overview: December 2014Dokument49 SeitenView Topic Percutaneous Coronary Intervention Overview: December 2014Siska Prima OlimvianiNoch keine Bewertungen
- Stress TestingDokument20 SeitenStress Testingaishwarya desaiNoch keine Bewertungen
- Athlete's Heart: Dr. Arzalan BaigDokument59 SeitenAthlete's Heart: Dr. Arzalan BaigArzalan BaigNoch keine Bewertungen
- Carotid Endarterectomy FinalDokument48 SeitenCarotid Endarterectomy Finalimad mokalledNoch keine Bewertungen
- Refrat VTDokument20 SeitenRefrat VTmuhammad ichsanNoch keine Bewertungen
- Chapter 80Dokument7 SeitenChapter 80annisarachmaNoch keine Bewertungen
- Cardiac TransplantDokument135 SeitenCardiac TransplantNakka SrikanthNoch keine Bewertungen
- Indikasi, Kontra Indikasi Serta Komplikasi Prosedur DiagnostikDokument54 SeitenIndikasi, Kontra Indikasi Serta Komplikasi Prosedur DiagnostikAnonymous QM0yMabNoch keine Bewertungen
- Heart Failure: Abdul Hafiz AliasDokument19 SeitenHeart Failure: Abdul Hafiz AliasAbdul Hafiz Alias100% (5)
- Coronary Vascular Disease: Focus On Coronary Artery Bypass GraftsDokument15 SeitenCoronary Vascular Disease: Focus On Coronary Artery Bypass Graftstrion_hNoch keine Bewertungen
- Basic Cardiac ImagingDokument40 SeitenBasic Cardiac ImagingSarah Sy-SantosNoch keine Bewertungen
- Cardiology: 27 Maret 2021Dokument52 SeitenCardiology: 27 Maret 2021Dian ParamitaNoch keine Bewertungen
- Medical Evaluation of Surgical Patient 2015049Dokument39 SeitenMedical Evaluation of Surgical Patient 2015049Kanneaufii KaramelNoch keine Bewertungen
- Pre-Operative Assessment of Cardiac Patients in Non Cardiac SurgeryDokument36 SeitenPre-Operative Assessment of Cardiac Patients in Non Cardiac SurgeryKush SurejaNoch keine Bewertungen
- Abdominal Aortic AneurysmDokument22 SeitenAbdominal Aortic Aneurysmatika5Noch keine Bewertungen
- Defibrillators in Nonischemic Cardiomyopathy Treatment EvaluationDokument7 SeitenDefibrillators in Nonischemic Cardiomyopathy Treatment EvaluationYanahi Oropeza HidalgoNoch keine Bewertungen
- MayoclinprocDokument12 SeitenMayoclinprocpriyaNoch keine Bewertungen
- Cardiovascular Problems in Long Term HemodialisisiDokument40 SeitenCardiovascular Problems in Long Term Hemodialisisifransiska wijoyoNoch keine Bewertungen
- Myocardial Perfusion ScanDokument47 SeitenMyocardial Perfusion ScanAkramNoch keine Bewertungen
- Shane P. Prejean, MD, Munaib Din, BSC, Eliana Reyes, MD, PHD, and Fadi G. Hage, MD, FasncDokument8 SeitenShane P. Prejean, MD, Munaib Din, BSC, Eliana Reyes, MD, PHD, and Fadi G. Hage, MD, FasncwidyadariNoch keine Bewertungen
- Master File 2003 - Body As A WholeDokument32 SeitenMaster File 2003 - Body As A Wholeobinna12Noch keine Bewertungen
- Preanesthetic Assessment of Cardiac Patients UndDokument42 SeitenPreanesthetic Assessment of Cardiac Patients UndParvathy R NairNoch keine Bewertungen
- Reno Vascular HypertensionDokument10 SeitenReno Vascular HypertensionAhmed Ali Mohammed AlbashirNoch keine Bewertungen
- Principle and Practice of Cardiac Mechanic For Assessing LV FunctionDokument33 SeitenPrinciple and Practice of Cardiac Mechanic For Assessing LV FunctionSofia Kusumadewi100% (1)
- Overview of Exercise Stress Testing: Annals of Saudi Medicine January 2006Dokument7 SeitenOverview of Exercise Stress Testing: Annals of Saudi Medicine January 2006Sari ChaerunisahNoch keine Bewertungen
- Handbook of Interventional Cardiac Procedures for Junior Cardiologists: A Summary of Current Cardiology LiteratureVon EverandHandbook of Interventional Cardiac Procedures for Junior Cardiologists: A Summary of Current Cardiology LiteratureNoch keine Bewertungen
- Management of Acute Ischemic Stroke.13Dokument10 SeitenManagement of Acute Ischemic Stroke.13Juan fernando Torres pavaNoch keine Bewertungen
- Limb IschaemiaDokument40 SeitenLimb Ischaemiaqaaneta bint-e-najafNoch keine Bewertungen
- GFZ 038Dokument3 SeitenGFZ 038adri20121989Noch keine Bewertungen
- CHP 11 Cerebral Air EmbolismDokument8 SeitenCHP 11 Cerebral Air EmbolismSrinivas GokulnathNoch keine Bewertungen
- Care of Clients With Neurologic Deficit: By: Elmer G. Organia, RNDokument233 SeitenCare of Clients With Neurologic Deficit: By: Elmer G. Organia, RNTina TalmadgeNoch keine Bewertungen
- Assessment and Management of StrokeDokument8 SeitenAssessment and Management of StrokeSiti Ariatus AyinaNoch keine Bewertungen
- Nursing Intervention : Been Experiencing Chest Pains)Dokument3 SeitenNursing Intervention : Been Experiencing Chest Pains)Czynna Dela CruzNoch keine Bewertungen
- Prevention For Neuromuscular Conditions: Brig (R) Ali Nasre AlamDokument26 SeitenPrevention For Neuromuscular Conditions: Brig (R) Ali Nasre AlamShimmering Moon100% (1)
- 2.best Insight Cardio Metabolic TeamDokument61 Seiten2.best Insight Cardio Metabolic TeamSaQlain BalochNoch keine Bewertungen
- Cerebrovascular AccidentDokument79 SeitenCerebrovascular AccidentKathy B. AbuanNoch keine Bewertungen
- Final 2021 Benefit Year Final HHS Risk Adjustment Model CoefficientsDokument26 SeitenFinal 2021 Benefit Year Final HHS Risk Adjustment Model CoefficientsJ CHANGNoch keine Bewertungen
- Upper Gastrointestinal - Esophageal BleedingDokument15 SeitenUpper Gastrointestinal - Esophageal Bleedingmardsz100% (9)
- Nursing Care Plan-1Dokument4 SeitenNursing Care Plan-1Sh3meeNoch keine Bewertungen
- Cell Injury 2Dokument23 SeitenCell Injury 2Cresha Mae PoloyapoyNoch keine Bewertungen
- Ischemic Heart DiseaseDokument116 SeitenIschemic Heart Diseasedrmsupriya09115983% (6)
- Surgery - 2020 With CorrectionDokument70 SeitenSurgery - 2020 With CorrectionBaraa KassisNoch keine Bewertungen
- Cardiovascular System Integrated Teaching ModuleDokument2 SeitenCardiovascular System Integrated Teaching ModuleShivan UmamaheswaranNoch keine Bewertungen
- Warfarin Mechanism of Action, Indications AtfDokument4 SeitenWarfarin Mechanism of Action, Indications AtfAmir mohammad moori MohammadiNoch keine Bewertungen
- Jalaukavacharana Medicinal Leech Therapy A Scientific Review in Ayurveda and BiomedicineDokument5 SeitenJalaukavacharana Medicinal Leech Therapy A Scientific Review in Ayurveda and BiomedicineEditor IJTSRDNoch keine Bewertungen
- The Mangled Extremity Score and Amputation Time FoDokument17 SeitenThe Mangled Extremity Score and Amputation Time FoTrisendi YogaNoch keine Bewertungen
- Minggu 3 Dr. Dr. Lisda MANAGEMENT ACUTE ISCHEMIC STROKEDokument47 SeitenMinggu 3 Dr. Dr. Lisda MANAGEMENT ACUTE ISCHEMIC STROKEPaten PisanNoch keine Bewertungen
- EFNS Congress Vienna Semax AbstractDokument60 SeitenEFNS Congress Vienna Semax AbstractnontjeNoch keine Bewertungen
- Health 8 3rd Quarter FinalDokument84 SeitenHealth 8 3rd Quarter FinalKrishia FelicesNoch keine Bewertungen
- Previous Exam Questions On NeuropsychiatryDokument2 SeitenPrevious Exam Questions On NeuropsychiatrymohamedNoch keine Bewertungen