Das könnte Ihnen auch gefallen
- How Do Humans Breathe? Science Book Age 8 | Children's Biology BooksVon EverandHow Do Humans Breathe? Science Book Age 8 | Children's Biology BooksNoch keine Bewertungen
- Thorax and Lung - LectureDokument60 SeitenThorax and Lung - LectureТаншолпан ШохбутоваNoch keine Bewertungen
- Pemeriksaan ThoraxDokument36 SeitenPemeriksaan ThoraxVaiz AhmadNoch keine Bewertungen
- Causes and Possible Prevention of Asthma and AllergiesVon EverandCauses and Possible Prevention of Asthma and AllergiesNoch keine Bewertungen
- Pemeriksaan ThoraxDokument27 SeitenPemeriksaan ThoraxYaasinta ArlaesNoch keine Bewertungen
- Breathe In, Breathe Out: Learning About Your LungsVon EverandBreathe In, Breathe Out: Learning About Your LungsBewertung: 3.5 von 5 Sternen3.5/5 (3)
- Pemeriksaan ThoraxDokument27 SeitenPemeriksaan ThoraxSubchanPrasetyoNoch keine Bewertungen
- Cardio AssessementDokument9 SeitenCardio AssessementPoonam soniNoch keine Bewertungen
- Terms RespiDokument5 SeitenTerms RespiDiane Kate Tobias MagnoNoch keine Bewertungen
- Encyclopaedia Britannica, 11th Edition, Volume 13, Slice 2 "Hearing" to "Helmond"Von EverandEncyclopaedia Britannica, 11th Edition, Volume 13, Slice 2 "Hearing" to "Helmond"Noch keine Bewertungen
- Respiratory Signs and SymptomsDokument11 SeitenRespiratory Signs and SymptomsChristiany Racho SalduaNoch keine Bewertungen
- Principles Auscultatory Areas: ND NDDokument5 SeitenPrinciples Auscultatory Areas: ND NDPinay YaunNoch keine Bewertungen
- Thorax and LungsDokument11 SeitenThorax and LungsJoel SantosNoch keine Bewertungen
- Lung SoundsDokument35 SeitenLung SoundsRaluca AndreeaNoch keine Bewertungen
- Pemeriksaan Fisik ThoraxDokument16 SeitenPemeriksaan Fisik ThoraxYudiWatanabeNoch keine Bewertungen
- Heart SoundsDokument20 SeitenHeart Soundsshd9617Noch keine Bewertungen
- CH 19-20Dokument8 SeitenCH 19-20yunqiwen2018Noch keine Bewertungen
- 8 Lung Auscultation Points and SoundsDokument11 Seiten8 Lung Auscultation Points and SoundsCHARIEMAE CA�AZARES100% (1)
- Heart Sounds & Murmurs ExamDokument4 SeitenHeart Sounds & Murmurs ExamSylheti BabaNoch keine Bewertungen
- Abnormal Breath SoundsDokument3 SeitenAbnormal Breath SoundsIndra PermanaNoch keine Bewertungen
- Chest & LungsDokument64 SeitenChest & LungsStudenteeNoch keine Bewertungen
- Abnormal Heart Sounds: First Heart Sound (S)Dokument4 SeitenAbnormal Heart Sounds: First Heart Sound (S)Faris Mufid MadyaputraNoch keine Bewertungen
- Final Death Note - Compre NotesDokument1.550 SeitenFinal Death Note - Compre NotesSteph TabasaNoch keine Bewertungen
- Heart SoundsDokument36 SeitenHeart SoundsRajveer100% (1)
- Cardiac Physical Exam and Innocent Murmurs PresentationDokument124 SeitenCardiac Physical Exam and Innocent Murmurs PresentationRajiv A. PatelNoch keine Bewertungen
- Pemeriksaan Thorax: Coass Interna RSI Sultan Agung SemarangDokument59 SeitenPemeriksaan Thorax: Coass Interna RSI Sultan Agung SemarangImada KhoironiNoch keine Bewertungen
- Heart Sounds and MurmursDokument38 SeitenHeart Sounds and MurmursLaura Moise100% (5)
- Heart SoundDokument29 SeitenHeart Sounddianpratiwirahim100% (1)
- Respiratory System-Review PathoDokument100 SeitenRespiratory System-Review PathoSadiePartington-RiopelleNoch keine Bewertungen
- Heart Sounds - PracticalDokument7 SeitenHeart Sounds - Practicalshadapaaak100% (1)
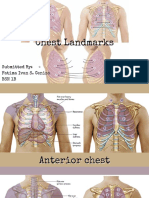
- Chest LandmarksDokument22 SeitenChest LandmarksFatima Ivan CenizaNoch keine Bewertungen
- Assessment of Lung and ChestDokument50 SeitenAssessment of Lung and ChestAbdurehman Ayele100% (1)
- Lung Sounds On Percussion and AuscultationDokument3 SeitenLung Sounds On Percussion and AuscultationKanika GuptaNoch keine Bewertungen
- Respiratory Maysa Fall2015 PDFDokument126 SeitenRespiratory Maysa Fall2015 PDFbaasheNoch keine Bewertungen
- Respi SystemDokument6 SeitenRespi SystemKalichandren ArumugamNoch keine Bewertungen
- Lung Examination: AbnormalDokument56 SeitenLung Examination: AbnormalBECAREFUL89ANoch keine Bewertungen
- IPPADokument4 SeitenIPPAIsaac KipchumbaNoch keine Bewertungen
- Thorax and Lungs ReferenceDokument8 SeitenThorax and Lungs Referencegwynth ripaldaNoch keine Bewertungen
- MVS Pulmonary AuscultationDokument8 SeitenMVS Pulmonary Auscultationvashini9151Noch keine Bewertungen
- MED 1.4 PE of The Chest, Lungs, Breast, and Axilla PDFDokument16 SeitenMED 1.4 PE of The Chest, Lungs, Breast, and Axilla PDFelleinasNoch keine Bewertungen
- Breathing SoundsDokument3 SeitenBreathing Soundsalthea jade villadonga100% (1)
- Clinical Findings in Respiratory SystemDokument1 SeiteClinical Findings in Respiratory SystemYusri ArifNoch keine Bewertungen
- Physical Examinations Respiratory System: InspectionDokument5 SeitenPhysical Examinations Respiratory System: InspectionAzizan HannyNoch keine Bewertungen
- The Thorax and Lungs - BATESDokument4 SeitenThe Thorax and Lungs - BATESsitalcoolk100% (2)
- PD 22 To 25Dokument96 SeitenPD 22 To 25Loai Mohammed IssaNoch keine Bewertungen
- Cardio AssessmentDokument2 SeitenCardio AssessmentMabesNoch keine Bewertungen
- 6 - Breath SoundsDokument31 Seiten6 - Breath SoundsggNoch keine Bewertungen
- Heart Sounds: Mitral Regurgitation Congestive Heart FailureDokument6 SeitenHeart Sounds: Mitral Regurgitation Congestive Heart FailurecindyNoch keine Bewertungen
- Heart SoundDokument16 SeitenHeart SoundAnggraeni Prameswari PutriNoch keine Bewertungen
- Chapter (10) : Assessment of Cardiovascular SystemDokument10 SeitenChapter (10) : Assessment of Cardiovascular SystemSandra GabasNoch keine Bewertungen
- Suara ParuDokument31 SeitenSuara ParuSuyanto nduduNoch keine Bewertungen
- The Breath Sounds: Intensity (Or Loudness)Dokument6 SeitenThe Breath Sounds: Intensity (Or Loudness)Santhosh KumarNoch keine Bewertungen
- Fisis Diagnositik IPDDokument96 SeitenFisis Diagnositik IPDMagfira Al HabsyiNoch keine Bewertungen
- Cardiovascular System-2Dokument71 SeitenCardiovascular System-2Aya AhmedNoch keine Bewertungen
- Physical Exam - Chest 2006Dokument84 SeitenPhysical Exam - Chest 2006api-19916399Noch keine Bewertungen
- Unit 06 Assessment of Thorax and LungDokument55 SeitenUnit 06 Assessment of Thorax and Lunghuma100% (1)
- 7th Heart Sounds and MurmursDokument6 Seiten7th Heart Sounds and MurmursbabibubeboNoch keine Bewertungen
- 3Dokument1 Seite3fajrinnnNoch keine Bewertungen
- Ria 1 Lplpo Obat JKN 2018-2019Dokument6 SeitenRia 1 Lplpo Obat JKN 2018-2019fajrinnnNoch keine Bewertungen
- 3Dokument1 Seite3fajrinnnNoch keine Bewertungen
- Nomor Sop, Uraian Tugas UkmDokument7 SeitenNomor Sop, Uraian Tugas UkmfajrinnnNoch keine Bewertungen
- Permenkes No 269 Tahun 2008 Rekam MedisDokument7 SeitenPermenkes No 269 Tahun 2008 Rekam MedisIstiqomah FlxNoch keine Bewertungen
- Professional Nursing OrganizationsDokument6 SeitenProfessional Nursing OrganizationsJohn Askof NyabutiNoch keine Bewertungen
- Single Dose VialsDokument54 SeitenSingle Dose VialsKyon Asma100% (1)
- Nauclea Latifolia: A Medicinal, Economic and Pharmacological ReviewDokument19 SeitenNauclea Latifolia: A Medicinal, Economic and Pharmacological ReviewMichael Kwesi BaahNoch keine Bewertungen
- Orthokeratology: Orthokeratology (Ortho-K) Is The Fitting of Specially Designed GasDokument4 SeitenOrthokeratology: Orthokeratology (Ortho-K) Is The Fitting of Specially Designed GasPUSHPAK DASGUPTANoch keine Bewertungen
- Pemeriksaan Thorax: Coass Interna RSI Sultan Agung SemarangDokument59 SeitenPemeriksaan Thorax: Coass Interna RSI Sultan Agung SemarangImada KhoironiNoch keine Bewertungen
- Factors Associated With Iron Deficiency Anemia Among Women of Childbearing Age in Yaqshid DistrictDokument82 SeitenFactors Associated With Iron Deficiency Anemia Among Women of Childbearing Age in Yaqshid DistrictMohamed Omar HassanNoch keine Bewertungen
- DR Swamy's Stations For Precourse PreparationDokument71 SeitenDR Swamy's Stations For Precourse PreparationdrsadafrafiNoch keine Bewertungen
- FHTMonitoringDokument21 SeitenFHTMonitoringlaarnie100% (1)
- Soal Ujian R2 FixedDokument9 SeitenSoal Ujian R2 Fixedprakoso jatiNoch keine Bewertungen
- Article With BhajanDokument4 SeitenArticle With BhajanBibek SutradharNoch keine Bewertungen
- Combinazioni SSC Unico PDFDokument73 SeitenCombinazioni SSC Unico PDFGiovanni PasqualiniNoch keine Bewertungen
- Ovarian Cancers The National Academies Press PDFDokument397 SeitenOvarian Cancers The National Academies Press PDFnersitiulfahNoch keine Bewertungen
- Rule 15Dokument2 SeitenRule 15begenyolNoch keine Bewertungen
- TUMOR MARKERS (Hand-Out) EDITDokument36 SeitenTUMOR MARKERS (Hand-Out) EDITAliza Dewi FortuaNoch keine Bewertungen
- Oral Meds ChecklistDokument2 SeitenOral Meds ChecklistMonika Sarmiento100% (1)
- Hip Vs SpineDokument12 SeitenHip Vs Spinevaibhav gowdaNoch keine Bewertungen
- Spasm of AccommdationDokument29 SeitenSpasm of Accommdationabdulaziz100% (1)
- 6 Birth DefectsDokument40 Seiten6 Birth DefectsjulieNoch keine Bewertungen
- RBC DisordersDokument70 SeitenRBC DisordersNdor Baribolo100% (1)
- FAQ On Blood DonationDokument2 SeitenFAQ On Blood DonationAnilNoch keine Bewertungen
- Intake Form: Health Declaration For TravellersDokument1 SeiteIntake Form: Health Declaration For TravellersJirir vimNoch keine Bewertungen
- Bacte01 STREPTOCOCCUS ENTEROCOCCUSDokument8 SeitenBacte01 STREPTOCOCCUS ENTEROCOCCUSAngelic AngelesNoch keine Bewertungen
- Eurican Technicalsheet 12-08-2019Dokument2 SeitenEurican Technicalsheet 12-08-2019dzulfikarfaizin romasNoch keine Bewertungen
- Arbeitsheft 2018Dokument147 SeitenArbeitsheft 2018Pamela MusabelliuNoch keine Bewertungen
- Gharama Za Matibabu PKP Kituo Cha AfyaDokument14 SeitenGharama Za Matibabu PKP Kituo Cha AfyashaggyzegratNoch keine Bewertungen
- Computed Tomography Radiation Safety Issues in OntarioDokument71 SeitenComputed Tomography Radiation Safety Issues in Ontariopebbles18950% (2)
- Hospitals in Coimbatore PDFDokument24 SeitenHospitals in Coimbatore PDFSACHIDANANDA SNoch keine Bewertungen
- Questionário Ii - Fundamentos Etimológicos Do InglêsDokument4 SeitenQuestionário Ii - Fundamentos Etimológicos Do InglêsDébora Bandeira David100% (1)
- Anti Human+HLA DR 174yb - 3174023DDokument1 SeiteAnti Human+HLA DR 174yb - 3174023DPaulo MattosNoch keine Bewertungen
- PediatricsDokument33 SeitenPediatricsnageshwarioshNoch keine Bewertungen