Das könnte Ihnen auch gefallen
- Adult Infectious Disease Bulletpoints HandbookVon EverandAdult Infectious Disease Bulletpoints HandbookBewertung: 4.5 von 5 Sternen4.5/5 (9)
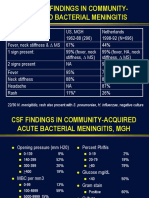
- Clinical Findings in Community-Acquired Bacterial MeningitisDokument35 SeitenClinical Findings in Community-Acquired Bacterial MeningitisMhelshy VillanuevaNoch keine Bewertungen
- Peppercorn Mesisskkknnn6Dokument33 SeitenPeppercorn Mesisskkknnn6Mhelshy VillanuevaNoch keine Bewertungen
- Managing Acute Meningitis: HistoryDokument37 SeitenManaging Acute Meningitis: HistoryMhelshy VillanuevaNoch keine Bewertungen
- Peppercorn Mesisskkknnn2Dokument38 SeitenPeppercorn Mesisskkknnn2Mhelshy VillanuevaNoch keine Bewertungen
- Diagnosis and Management of Acute Bacterial MeningitisDokument47 SeitenDiagnosis and Management of Acute Bacterial MeningitisMhelshy VillanuevaNoch keine Bewertungen
- What Does He Have?: Questions To AddressDokument43 SeitenWhat Does He Have?: Questions To AddressMhelshy VillanuevaNoch keine Bewertungen
- Case Example: Presents For Evaluation When He Starts To Notice Faint Rash On Trunk, Back and Arms No Known Sick ContactsDokument46 SeitenCase Example: Presents For Evaluation When He Starts To Notice Faint Rash On Trunk, Back and Arms No Known Sick ContactsMhelshy VillanuevaNoch keine Bewertungen
- Peppercorn MesDokument44 SeitenPeppercorn MesMhelshy VillanuevaNoch keine Bewertungen
- Etiologies of Single Episode Acute Bacterial Meningitis, MGH 1962-88Dokument41 SeitenEtiologies of Single Episode Acute Bacterial Meningitis, MGH 1962-88Mhelshy VillanuevaNoch keine Bewertungen
- Meningitis 2005Dokument87 SeitenMeningitis 2005nafisyarifahNoch keine Bewertungen
- Community Acquired Bacterial Meningitis in AdultsDokument45 SeitenCommunity Acquired Bacterial Meningitis in AdultsDaniel Tettamanti MirandaNoch keine Bewertungen
- Central Nervous System Infections 2024Dokument41 SeitenCentral Nervous System Infections 2024aguilarjanicaNoch keine Bewertungen
- Demam NeutropeniaDokument35 SeitenDemam Neutropeniaariz setiNoch keine Bewertungen
- Meningitis and Encephalitis: PGI Roddame Angelo ErispeDokument100 SeitenMeningitis and Encephalitis: PGI Roddame Angelo ErispeAngelo ErispeNoch keine Bewertungen
- Approach To Meningitis and EncephalitisDokument40 SeitenApproach To Meningitis and EncephalitisDrvicky BaxiNoch keine Bewertungen
- Sterile Body Fluids: Brett CrawleyDokument21 SeitenSterile Body Fluids: Brett CrawleydewiNoch keine Bewertungen
- MENINGITIS DR Syad Akram Ali 01-12-2014Dokument95 SeitenMENINGITIS DR Syad Akram Ali 01-12-2014Gopireddy Sivakarthik ReddyNoch keine Bewertungen
- Grand Round July 2019Dokument61 SeitenGrand Round July 2019Arslan Rahat UllahNoch keine Bewertungen
- Meningitis AND Encephalitis: by DR .. Magdi Elbaloola Ahmed Physcian & GastrohepatologistDokument51 SeitenMeningitis AND Encephalitis: by DR .. Magdi Elbaloola Ahmed Physcian & GastrohepatologistÅbübâkêř Äbd-ëřhēēm BãřřîNoch keine Bewertungen
- Meningitis Pathophysiology PDFDokument59 SeitenMeningitis Pathophysiology PDFpaswordnyalupa100% (1)
- Acute CNS Infections: James E. Peacock, Jr. MDDokument53 SeitenAcute CNS Infections: James E. Peacock, Jr. MDEhab KhiryNoch keine Bewertungen
- 13 Meningitis Beyond Neonatal AgeDokument57 Seiten13 Meningitis Beyond Neonatal AgeABDELA DAFO IJARONoch keine Bewertungen
- (K8) Sepsis Kuliah 2016Dokument37 Seiten(K8) Sepsis Kuliah 2016mayastplNoch keine Bewertungen
- Acute Bacterial MeningitiDokument31 SeitenAcute Bacterial MeningitiHesbon MomanyiNoch keine Bewertungen
- BM 2.3 Bambang SudarmantoDokument46 SeitenBM 2.3 Bambang SudarmantoAbdullah ShiddiqNoch keine Bewertungen
- Meningitis: Presented By:dr. Alaa Nugud ABH-Medical DepartmentDokument23 SeitenMeningitis: Presented By:dr. Alaa Nugud ABH-Medical DepartmentALaa NugudNoch keine Bewertungen
- Rahma Dan CAPDokument17 SeitenRahma Dan CAPpeterNoch keine Bewertungen
- Febrile Neutropenia Final 7-29Dokument74 SeitenFebrile Neutropenia Final 7-29Juliyanti FuNoch keine Bewertungen
- Ventilator: Associated Pneumonia (VAP)Dokument36 SeitenVentilator: Associated Pneumonia (VAP)D. Melba S.S ChinnaNoch keine Bewertungen
- Triject - Cap & HapDokument34 SeitenTriject - Cap & Hapmaliakbar111Noch keine Bewertungen
- DR .Praveen NagulaDokument40 SeitenDR .Praveen NagulaPordil KhanNoch keine Bewertungen
- Sdidjas, Spa (K) Prof - DR.HJ - Rafita Ramayati, Spa (K) DR - Hj.Oke Rina Ramayani, Spa Dept - Ika Fk-Uisu - J Alan SM Raja No. 2A, MedanDokument53 SeitenSdidjas, Spa (K) Prof - DR.HJ - Rafita Ramayati, Spa (K) DR - Hj.Oke Rina Ramayani, Spa Dept - Ika Fk-Uisu - J Alan SM Raja No. 2A, Medanernawaty nadeakNoch keine Bewertungen
- CNSInfections 2Dokument39 SeitenCNSInfections 2Nica BalaresNoch keine Bewertungen
- Meningitis Beyond The Neonatal AgeDokument51 SeitenMeningitis Beyond The Neonatal AgeBeamlak Getachew WoldeselassieNoch keine Bewertungen
- CeftriaxoneDokument60 SeitenCeftriaxoneHuggerNoch keine Bewertungen
- Atypical PneumoniaDokument76 SeitenAtypical PneumoniaRiski DohartuaNoch keine Bewertungen
- Oncologic EmergenciesDokument43 SeitenOncologic Emergencieshernandez2812Noch keine Bewertungen
- Acute CNS InfectionsDokument46 SeitenAcute CNS InfectionsLily SolNoch keine Bewertungen
- Infeksi Pada Pasien KankerDokument18 SeitenInfeksi Pada Pasien KankerSuci Fitriani SammuliaNoch keine Bewertungen
- Meningitis, Encephalitis and Brain Abscess: by D OgoinaDokument62 SeitenMeningitis, Encephalitis and Brain Abscess: by D OgoinaPrincewill SeiyefaNoch keine Bewertungen
- Clabsi DR - RonaldDokument19 SeitenClabsi DR - RonaldsilviNoch keine Bewertungen
- Siu Empiric Antibiotics For Select InfectionsDokument30 SeitenSiu Empiric Antibiotics For Select InfectionspasswordNoch keine Bewertungen
- Varicella Infection What Kind of Virus Is It? How Does It Get Around?Dokument2 SeitenVaricella Infection What Kind of Virus Is It? How Does It Get Around?introvoyz041Noch keine Bewertungen
- 2.fahad Khaliq.... Febrile Neutro - pptx-1Dokument38 Seiten2.fahad Khaliq.... Febrile Neutro - pptx-1dr FAHADKHALIQSIALNoch keine Bewertungen
- 2.fahad Khaliq.... Febrile Neutro - pptx-1Dokument38 Seiten2.fahad Khaliq.... Febrile Neutro - pptx-1dr FAHADKHALIQSIALNoch keine Bewertungen
- Neumonías 2008Dokument62 SeitenNeumonías 2008Lucero BautistaNoch keine Bewertungen
- PNEUMONIADokument5 SeitenPNEUMONIARafael KameradNoch keine Bewertungen
- Approaches To Febrile Neutropenia 2011 IDSA-ECIL GuidelinesDokument24 SeitenApproaches To Febrile Neutropenia 2011 IDSA-ECIL GuidelinesHusein AssagafNoch keine Bewertungen
- Harrison 164 - MeningitisDokument2 SeitenHarrison 164 - MeningitisChristel GarciaNoch keine Bewertungen
- Sepsis: George C. Mejicano, MD Department of Medicine University of WisconsinDokument50 SeitenSepsis: George C. Mejicano, MD Department of Medicine University of WisconsincupacupuNoch keine Bewertungen
- Neutropenia BroshureDokument2 SeitenNeutropenia BroshurenicoleshawnutritionNoch keine Bewertungen
- Pneumonia in Critical Patients - KARTIKADokument29 SeitenPneumonia in Critical Patients - KARTIKAKartika JuwitaNoch keine Bewertungen
- CSF Findings in MeningitisDokument11 SeitenCSF Findings in MeningitisLioraNoch keine Bewertungen
- Bacterial Meningitis: Objectives: Wayne L. Gold, MDDokument11 SeitenBacterial Meningitis: Objectives: Wayne L. Gold, MDAtikah Na'aimNoch keine Bewertungen
- Recent Update in The Management of Invasive Fungal InfectionDokument30 SeitenRecent Update in The Management of Invasive Fungal Infectionanoop61100% (2)
- Meningitis TopicDokument9 SeitenMeningitis Topicapi-668691030Noch keine Bewertungen
- 1100 - Lee PneumoniasDokument37 Seiten1100 - Lee PneumoniasAlejandro Kanito Alvarez SNoch keine Bewertungen
- Meningitis PresentationDokument41 SeitenMeningitis PresentationO'Mark AndrewsNoch keine Bewertungen
- B.3.aamelita D. Balliao - Lupang Hinirang - Group 3Dokument1 SeiteB.3.aamelita D. Balliao - Lupang Hinirang - Group 3Mhelshy VillanuevaNoch keine Bewertungen
- 2 CoVID-19 Case Investigation Form PDFDokument1 Seite2 CoVID-19 Case Investigation Form PDFMhelshy VillanuevaNoch keine Bewertungen
- BreakfastDokument1 SeiteBreakfastMhelshy VillanuevaNoch keine Bewertungen
- KS4 Physical Education: The Circulatory SystemDokument36 SeitenKS4 Physical Education: The Circulatory SystemAjay Pal NattNoch keine Bewertungen
- BreakfastDokument1 SeiteBreakfastMhelshy VillanuevaNoch keine Bewertungen
- Anti Bullying For Children PDF VersionDokument2 SeitenAnti Bullying For Children PDF VersionMhelshy VillanuevaNoch keine Bewertungen
- Peppercorn MesisskkknnnDokument40 SeitenPeppercorn MesisskkknnnMhelshy VillanuevaNoch keine Bewertungen
- B.2.a.cindy G. Awe - Concrete Poetry - Group 3Dokument1 SeiteB.2.a.cindy G. Awe - Concrete Poetry - Group 3Mhelshy VillanuevaNoch keine Bewertungen
- Peppercorn MesisskkknnnDokument40 SeitenPeppercorn MesisskkknnnMhelshy VillanuevaNoch keine Bewertungen
- Peppercorn MesissDokument42 SeitenPeppercorn MesissMhelshy VillanuevaNoch keine Bewertungen
- Etiologies of Single Episode Acute Bacterial Meningitis, MGH 1962-88Dokument41 SeitenEtiologies of Single Episode Acute Bacterial Meningitis, MGH 1962-88Mhelshy VillanuevaNoch keine Bewertungen
- Case Example: Presents For Evaluation When He Starts To Notice Faint Rash On Trunk, Back and Arms No Known Sick ContactsDokument46 SeitenCase Example: Presents For Evaluation When He Starts To Notice Faint Rash On Trunk, Back and Arms No Known Sick ContactsMhelshy VillanuevaNoch keine Bewertungen
- Peppercorn MeDokument45 SeitenPeppercorn MeMhelshy VillanuevaNoch keine Bewertungen
- Peppercorn MesDokument44 SeitenPeppercorn MesMhelshy VillanuevaNoch keine Bewertungen
- What Does He Have?: Questions To AddressDokument43 SeitenWhat Does He Have?: Questions To AddressMhelshy VillanuevaNoch keine Bewertungen
- History of ChemistryDokument4 SeitenHistory of ChemistryMhelshy VillanuevaNoch keine Bewertungen
- History of ChemistryDokument4 SeitenHistory of ChemistryMhelshy VillanuevaNoch keine Bewertungen
- Midwifery Program CatalogueDokument20 SeitenMidwifery Program CatalogueMhelshy Villanueva100% (1)
- Bayangan-Milo Nuptial Narciso & NoemiDokument2 SeitenBayangan-Milo Nuptial Narciso & NoemiMhelshy VillanuevaNoch keine Bewertungen
- History of Iglesia Ni Cristo: Is Christ God?Dokument2 SeitenHistory of Iglesia Ni Cristo: Is Christ God?Mhelshy VillanuevaNoch keine Bewertungen
- IISFM Schemes PDFDokument1 SeiteIISFM Schemes PDFSurendrasinghNoch keine Bewertungen
- Mh25 Borderline Personality GuidelineDokument182 SeitenMh25 Borderline Personality GuidelineAbdul Hakim Abdul KadirNoch keine Bewertungen
- KT PDO Thread Training Stage 1 and 2 OverviewDokument55 SeitenKT PDO Thread Training Stage 1 and 2 OverviewMetin Sabuncu100% (3)
- CCAC MSW City Action Plan Cebu City, PhilippinesDokument6 SeitenCCAC MSW City Action Plan Cebu City, Philippinesca1Noch keine Bewertungen
- Specification Sheet: Product: Salted Anchovy in BarrelsDokument1 SeiteSpecification Sheet: Product: Salted Anchovy in BarrelsPoesía PeruanaNoch keine Bewertungen
- Modified SAD PERSONS ScaleDokument1 SeiteModified SAD PERSONS ScaleValeria ShimbomehNoch keine Bewertungen
- 1823 - Part - A - DCHB - Kamrup Metropolitan PDFDokument224 Seiten1823 - Part - A - DCHB - Kamrup Metropolitan PDFSaddam FaruqueNoch keine Bewertungen
- QA/QC of Nuclear Medicine Imaging Equipment - Current PracticesDokument38 SeitenQA/QC of Nuclear Medicine Imaging Equipment - Current PracticesRosendo DacuyanNoch keine Bewertungen
- Smartphones and Sleep - MediaDokument2 SeitenSmartphones and Sleep - Mediaivan7tatNoch keine Bewertungen
- Umbilical Cord Blood BankingDokument290 SeitenUmbilical Cord Blood BankingcmNoch keine Bewertungen
- Lazuli ProfileDokument25 SeitenLazuli ProfileNew Seljuk EmpireNoch keine Bewertungen
- Basic Maternity ConceptsDokument14 SeitenBasic Maternity ConceptsDivine Grace Arreglo AbingNoch keine Bewertungen
- Tarea 2.: Ingles 5.1 Fernano Boluda Del PinoDokument2 SeitenTarea 2.: Ingles 5.1 Fernano Boluda Del PinoFernando Boluda Del PinoNoch keine Bewertungen
- PLLDokument24 SeitenPLLjagannnathdNoch keine Bewertungen
- UltraCal XS PDFDokument2 SeitenUltraCal XS PDFKarina OjedaNoch keine Bewertungen
- Test I. True or False. Write TRUE If The Statement Is Correct and FALSE If The Statement Is IncorrectDokument2 SeitenTest I. True or False. Write TRUE If The Statement Is Correct and FALSE If The Statement Is IncorrectMariecris Barayuga Duldulao-AbelaNoch keine Bewertungen
- 11 - Chapter 3Dokument52 Seiten11 - Chapter 3joshniNoch keine Bewertungen
- How Human Microbiome Talks To Health and DiseaseDokument7 SeitenHow Human Microbiome Talks To Health and DiseaseRafa SotoNoch keine Bewertungen
- PDFDokument278 SeitenPDFmahesh babu100% (1)
- Master Form JSADokument2 SeitenMaster Form JSAAgung PrasetyooNoch keine Bewertungen
- Tree of LifeDokument909 SeitenTree of LifeMariza D. KabamaruNoch keine Bewertungen
- Schedule of Charges-Holy Family - Sep 08Dokument64 SeitenSchedule of Charges-Holy Family - Sep 08Quirinevv100% (1)
- The Superheroes of PharmaDokument13 SeitenThe Superheroes of PharmaMPANoch keine Bewertungen
- The Intentional Application of Humor With CKD PatientsDokument8 SeitenThe Intentional Application of Humor With CKD PatientsKaryn BuxmanNoch keine Bewertungen
- AbraDokument4 SeitenAbralhhjklllNoch keine Bewertungen
- TST Referral Form v.2Dokument3 SeitenTST Referral Form v.2John Philip TiongcoNoch keine Bewertungen
- Gastro-Intestinal Tract: Entamoeba HistolyticaDokument25 SeitenGastro-Intestinal Tract: Entamoeba Histolyticanh2411Noch keine Bewertungen
- Paintball City Waiver FormDokument1 SeitePaintball City Waiver FormAndrew HalsteadNoch keine Bewertungen
- Kacee-New ResumeDokument4 SeitenKacee-New Resumeapi-678307618Noch keine Bewertungen
- Monkeypox: VirusDokument18 SeitenMonkeypox: Virusdiela dwi lestariNoch keine Bewertungen