Das könnte Ihnen auch gefallen
- Immediate Life Support for healthcare Practitioners: A Step-By-Step GuideVon EverandImmediate Life Support for healthcare Practitioners: A Step-By-Step GuideNoch keine Bewertungen
- Cardiovascular Examination FinalDokument28 SeitenCardiovascular Examination FinalAllen Caine Taabbil100% (1)
- Cardiovascular History Taking and Physical ExaminationsDokument35 SeitenCardiovascular History Taking and Physical ExaminationsEndalk AsfawNoch keine Bewertungen
- CVS Examination InstructionsDokument5 SeitenCVS Examination Instructionsmagdy balahaNoch keine Bewertungen
- CardiovascularDokument1 SeiteCardiovascularshellstyneyenyenNoch keine Bewertungen
- Cardiovascular Assessment (1) - StudentsDokument70 SeitenCardiovascular Assessment (1) - Studentsraima ayazNoch keine Bewertungen
- Assessment of CvsDokument70 SeitenAssessment of CvsTouseeq ManzoorNoch keine Bewertungen
- Cardiovascular Assessment (1)Dokument73 SeitenCardiovascular Assessment (1)matthewsarfrazbhattiNoch keine Bewertungen
- Assessment of Caridovascular SysDokument36 SeitenAssessment of Caridovascular Syssceince with EZNoch keine Bewertungen
- History and Examinatoin of The Cardiovascular SystemDokument47 SeitenHistory and Examinatoin of The Cardiovascular Systemmawada abdallaNoch keine Bewertungen
- Cardiovascular Examination:: General InspectionDokument6 SeitenCardiovascular Examination:: General InspectionPhysician AssociateNoch keine Bewertungen
- Assessment Cardiovascular System 2Dokument24 SeitenAssessment Cardiovascular System 2TASNEEM LAKKADSHANoch keine Bewertungen
- Clinical Examination - Eric Sarpong-NtiamoahDokument52 SeitenClinical Examination - Eric Sarpong-NtiamoahFathimathNoch keine Bewertungen
- Osce Notes - Rac - Safina AdatiaDokument35 SeitenOsce Notes - Rac - Safina AdatiaTraventure 2000Noch keine Bewertungen
- Checklist For Examination of The Cardiovascular SystemDokument15 SeitenChecklist For Examination of The Cardiovascular SystemAzizan Hanny100% (1)
- CardiacassessmentDokument40 SeitenCardiacassessmentsasNoch keine Bewertungen
- Cardiovascular Physical Examination GuideDokument59 SeitenCardiovascular Physical Examination GuideSheila Jessica AndavaniaNoch keine Bewertungen
- Vital Signs Examination - Kuliah SMT 2 2008Dokument54 SeitenVital Signs Examination - Kuliah SMT 2 2008VilasineeAriHaraKumarNoch keine Bewertungen
- Clinical Skills Handbook 2015 MEDN40060 2Dokument66 SeitenClinical Skills Handbook 2015 MEDN40060 2Wilson KhawNoch keine Bewertungen
- Heart & Neck Vessel AssessmentDokument46 SeitenHeart & Neck Vessel AssessmentLouise Nathalia VelasquezNoch keine Bewertungen
- Big Three ExamsDokument17 SeitenBig Three Examszulaikhaa.bbNoch keine Bewertungen
- Cardiovascular ExaminationDokument54 SeitenCardiovascular ExaminationsankethNoch keine Bewertungen
- Approach To Patients With Possible Cardiovascular Disease and Physical Examination of The Cardiovascular SystemDokument79 SeitenApproach To Patients With Possible Cardiovascular Disease and Physical Examination of The Cardiovascular SystemLajel S. LachicaNoch keine Bewertungen
- Assessment Cardiovascular Sy - 1Dokument32 SeitenAssessment Cardiovascular Sy - 1TASNEEM LAKKADSHANoch keine Bewertungen
- Cardiacassessmentppt 170323092148Dokument48 SeitenCardiacassessmentppt 170323092148sasNoch keine Bewertungen
- Cardiac Exam Guide for CliniciansDokument5 SeitenCardiac Exam Guide for CliniciansAmit MartinNoch keine Bewertungen
- Physical DiagnosisDokument97 SeitenPhysical Diagnosisaxmedfare138Noch keine Bewertungen
- Kuliah Pemeriksaan Fisik CVDokument49 SeitenKuliah Pemeriksaan Fisik CVAyu BintangNoch keine Bewertungen
- Lab 5 Cardiovascular Examination, ECG and BPDokument43 SeitenLab 5 Cardiovascular Examination, ECG and BP202310446Noch keine Bewertungen
- Respiratory Failure Results From Inadequate Gas ExchangeDokument7 SeitenRespiratory Failure Results From Inadequate Gas ExchangeJiezl Abellano AfinidadNoch keine Bewertungen
- Cardiovascular ExaminationDokument5 SeitenCardiovascular ExaminationMTBRISCOENoch keine Bewertungen
- Cardiovascular Examination GuideDokument2 SeitenCardiovascular Examination Guiderhea100% (1)
- Pemeriksaan Tanda Vital-Kuliah PengantarDokument22 SeitenPemeriksaan Tanda Vital-Kuliah PengantarDwitia IswariNoch keine Bewertungen
- Cardio ExamDokument3 SeitenCardio ExamImperial HinduSocNoch keine Bewertungen
- Examination and Investigation of The Cardiovascular System (CVS)Dokument27 SeitenExamination and Investigation of The Cardiovascular System (CVS)Jake MillerNoch keine Bewertungen
- Cardiac ExaminationDokument21 SeitenCardiac ExaminationPraneetha NouduriNoch keine Bewertungen
- 3 - Vital SignDokument27 Seiten3 - Vital SignBav VAansoqnuaetzNoch keine Bewertungen
- Lung Expansion RevisionDokument89 SeitenLung Expansion RevisionPatrick RoqueNoch keine Bewertungen
- Chest CaseDokument19 SeitenChest CaseNesma AdelNoch keine Bewertungen
- Physical DiagnosisDokument63 SeitenPhysical Diagnosishailemariamgebrehiwot02Noch keine Bewertungen
- New HematologyOncology FAE2016Dokument108 SeitenNew HematologyOncology FAE2016omarNoch keine Bewertungen
- Peripheral Arterial Pulse and JVP: Sweta Sah Intern JMCTHDokument40 SeitenPeripheral Arterial Pulse and JVP: Sweta Sah Intern JMCTHsahsweta67Noch keine Bewertungen
- Cvs PracticalDokument63 SeitenCvs PracticalSreedeep TejaNoch keine Bewertungen
- Chapter 07 Taking Vital SignsDokument22 SeitenChapter 07 Taking Vital SignsNephNoch keine Bewertungen
- Assessment of the Cardiovascular SystemDokument61 SeitenAssessment of the Cardiovascular SystemYunus ElonNoch keine Bewertungen
- Case Study I: Observation of A Case in Emergency Department For Diagnosis & ManagementDokument6 SeitenCase Study I: Observation of A Case in Emergency Department For Diagnosis & ManagementAbdulrahman Mohamed GhanimNoch keine Bewertungen
- Cardiovascular BigDokument37 SeitenCardiovascular Bigfaiz nasirNoch keine Bewertungen
- Principles in Trauma ManagementDokument34 SeitenPrinciples in Trauma Managementvirz23Noch keine Bewertungen
- Cardiopulmonary PT Assessment For1 Note - 230327 - 000213 PDFDokument7 SeitenCardiopulmonary PT Assessment For1 Note - 230327 - 000213 PDFTanoy SutradharNoch keine Bewertungen
- Cardiovascular System: Jonalyn Sotero Esco RN., MANDokument122 SeitenCardiovascular System: Jonalyn Sotero Esco RN., MANClifford Subagan Patil-aoNoch keine Bewertungen
- Physical DiagnosisDokument42 SeitenPhysical DiagnosisKhim Yalong100% (1)
- Fundamentals Vital Signs ReviewDokument94 SeitenFundamentals Vital Signs Reviewymitchell7Noch keine Bewertungen
- Basic Physical Assessment 1Dokument62 SeitenBasic Physical Assessment 1Janry-Mae Escobar TumanengNoch keine Bewertungen
- Approach To The Cardiovascular Examination567 160120085414 PDFDokument22 SeitenApproach To The Cardiovascular Examination567 160120085414 PDFHNINNoch keine Bewertungen
- Anesthesia Techniques for Cesarean SectionDokument70 SeitenAnesthesia Techniques for Cesarean SectionElsya ParamitasariNoch keine Bewertungen
- Presentation B. INGGRIS FIKS BUK PUPUTDokument52 SeitenPresentation B. INGGRIS FIKS BUK PUPUTRosy OktaridaNoch keine Bewertungen
- Medicine 1 Final Practical Exam ReviewerDokument10 SeitenMedicine 1 Final Practical Exam ReviewerTP RMadNoch keine Bewertungen
- 2.8 09 S002-General Notes - Sheet 2 - 02 PDFDokument1 Seite2.8 09 S002-General Notes - Sheet 2 - 02 PDFSaiful IslamNoch keine Bewertungen
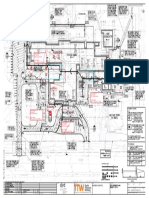
- Mark Up Basement and Footing ConcordDokument2 SeitenMark Up Basement and Footing ConcordSaiful IslamNoch keine Bewertungen
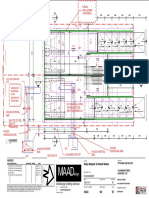
- MARK UP Ground SlabDokument1 SeiteMARK UP Ground SlabSaiful IslamNoch keine Bewertungen
- Lot 4 DP 1274443 ShedDokument1 SeiteLot 4 DP 1274443 ShedSaiful IslamNoch keine Bewertungen
- B1, Timber Beam Analysis & Design (AS1720)Dokument3 SeitenB1, Timber Beam Analysis & Design (AS1720)Saiful IslamNoch keine Bewertungen
- J0535-S004 - Crane Radius Plan PDFDokument1 SeiteJ0535-S004 - Crane Radius Plan PDFSaiful IslamNoch keine Bewertungen
- B1, Timber Beam Analysis & Design (AS1720)Dokument3 SeitenB1, Timber Beam Analysis & Design (AS1720)Saiful IslamNoch keine Bewertungen
- B1, Timber Beam Analysis & Design (AS1720)Dokument3 SeitenB1, Timber Beam Analysis & Design (AS1720)Saiful IslamNoch keine Bewertungen
- B1, Timber Beam Analysis & Design (AS1720)Dokument3 SeitenB1, Timber Beam Analysis & Design (AS1720)Saiful IslamNoch keine Bewertungen
- G0526202 1775 Cogs PDFDokument1 SeiteG0526202 1775 Cogs PDFSaiful IslamNoch keine Bewertungen
- J0535-S003 - Crane Footing Plan PDFDokument1 SeiteJ0535-S003 - Crane Footing Plan PDFSaiful IslamNoch keine Bewertungen
- J0535-S002 - Crane Elevation PDFDokument1 SeiteJ0535-S002 - Crane Elevation PDFSaiful IslamNoch keine Bewertungen
- J0535-S001 - General Notes PDFDokument1 SeiteJ0535-S001 - General Notes PDFSaiful IslamNoch keine Bewertungen
- DA Consent PDFDokument16 SeitenDA Consent PDFSaiful IslamNoch keine Bewertungen
- Appendix Q Geotechnical InvestigationDokument43 SeitenAppendix Q Geotechnical InvestigationSaiful IslamNoch keine Bewertungen
- Slab Layout: DWG No 190811 DDokument14 SeitenSlab Layout: DWG No 190811 DSaiful IslamNoch keine Bewertungen
- 36-40 Kenyon Street, Fairfield, MRT48-36m-MRT48-36 Plan ViewDokument1 Seite36-40 Kenyon Street, Fairfield, MRT48-36m-MRT48-36 Plan ViewSaiful IslamNoch keine Bewertungen
- Pay SlipDokument1 SeitePay SlipSaiful IslamNoch keine Bewertungen
- S16-013 - Variation 725 - Bowen Place Parkes Pile Cage - Design CertificateDokument2 SeitenS16-013 - Variation 725 - Bowen Place Parkes Pile Cage - Design CertificateSaiful IslamNoch keine Bewertungen
- Cad DrawingDokument53 SeitenCad DrawingAvish Gunnuck100% (3)
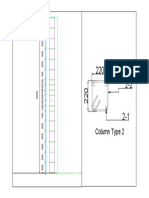
- Column Type 2Dokument1 SeiteColumn Type 2Saiful IslamNoch keine Bewertungen
- ApplicationDokument3 SeitenApplicationSaiful IslamNoch keine Bewertungen
- Splice Joint 100Dokument4 SeitenSplice Joint 100Saiful IslamNoch keine Bewertungen
- Column RetorDokument1 SeiteColumn RetorSaiful IslamNoch keine Bewertungen
- Splice Joint 100Dokument1 SeiteSplice Joint 100Saiful IslamNoch keine Bewertungen
- Pay SlipDokument1 SeitePay SlipSaiful IslamNoch keine Bewertungen
- Steel UC Colm (When Only Compression, Axial Load) - Australia StandardDokument9 SeitenSteel UC Colm (When Only Compression, Axial Load) - Australia StandardSaiful IslamNoch keine Bewertungen
- Tekla Training StepDokument1 SeiteTekla Training StepSaiful IslamNoch keine Bewertungen
- Guidelines for Plumbing Rainwater TanksDokument9 SeitenGuidelines for Plumbing Rainwater TanksSaiful IslamNoch keine Bewertungen
- Queries Zone 2&3Dokument2 SeitenQueries Zone 2&3Saiful IslamNoch keine Bewertungen
- 1"a Study On Employee Retention in Amara Raja Power Systems LTDDokument81 Seiten1"a Study On Employee Retention in Amara Raja Power Systems LTDJerome Samuel100% (1)
- Clausius TheoremDokument3 SeitenClausius TheoremNitish KumarNoch keine Bewertungen
- The Art of Now: Six Steps To Living in The MomentDokument5 SeitenThe Art of Now: Six Steps To Living in The MomentGiovanni AlloccaNoch keine Bewertungen
- TILE QUOTEDokument3 SeitenTILE QUOTEHarsh SathvaraNoch keine Bewertungen
- O2 Orthodontic Lab Catalog PDFDokument20 SeitenO2 Orthodontic Lab Catalog PDFplayer osamaNoch keine Bewertungen
- F-16c.1 Ginkgo Ginkgolic AcidDokument2 SeitenF-16c.1 Ginkgo Ginkgolic AcidNarongchai PongpanNoch keine Bewertungen
- 2019 Course CatalogDokument31 Seiten2019 Course CatalogDeepen SharmaNoch keine Bewertungen
- Laser Surface Treatment ProcessesDokument63 SeitenLaser Surface Treatment ProcessesDIPAK VINAYAK SHIRBHATENoch keine Bewertungen
- مقدمةDokument5 SeitenمقدمةMahmoud MadanyNoch keine Bewertungen
- CP 343-1Dokument23 SeitenCP 343-1Yahya AdamNoch keine Bewertungen
- JK Paper Q4FY11 Earnings Call TranscriptDokument10 SeitenJK Paper Q4FY11 Earnings Call TranscriptkallllllooooNoch keine Bewertungen
- The Impact of Employees' Commitment Towards Food Safety at Ayana Resort, BaliDokument58 SeitenThe Impact of Employees' Commitment Towards Food Safety at Ayana Resort, Balirachelle agathaNoch keine Bewertungen
- Maureen L. Walsh - Re-Imagining Redemption. Universal Salvation in The Theology of Julian of NorwichDokument20 SeitenMaureen L. Walsh - Re-Imagining Redemption. Universal Salvation in The Theology of Julian of NorwichAni LupascuNoch keine Bewertungen
- Reflection 2: WHAT DOES It Mean To Be A Pacific Islander Today and in The Future To Me?Dokument5 SeitenReflection 2: WHAT DOES It Mean To Be A Pacific Islander Today and in The Future To Me?Trishika NamrataNoch keine Bewertungen
- Canon imageFORMULA DR-X10CDokument208 SeitenCanon imageFORMULA DR-X10CYury KobzarNoch keine Bewertungen
- Letter of MotivationDokument4 SeitenLetter of Motivationjawad khalidNoch keine Bewertungen
- Effective Time ManagementDokument61 SeitenEffective Time ManagementTafadzwa94% (16)
- Oral Nutrition Support NotesDokument28 SeitenOral Nutrition Support Notesleemon.mary.alipao8695Noch keine Bewertungen
- The Apu Trilogy - Robin Wood PDFDokument48 SeitenThe Apu Trilogy - Robin Wood PDFSamkush100% (1)
- Motor Wiring Diagram: D.C. Motor ConnectionsDokument1 SeiteMotor Wiring Diagram: D.C. Motor Connectionsczds6594Noch keine Bewertungen
- Aacra Draft Preliminary Report PDFDokument385 SeitenAacra Draft Preliminary Report PDFBeselam SeyedNoch keine Bewertungen
- Diia Specification: Dali Part 252 - Energy ReportingDokument15 SeitenDiia Specification: Dali Part 252 - Energy Reportingtufta tuftaNoch keine Bewertungen
- Maintenance Handbook On Compressors (Of Under Slung AC Coaches) PDFDokument39 SeitenMaintenance Handbook On Compressors (Of Under Slung AC Coaches) PDFSandeepNoch keine Bewertungen
- Rectifiers and FiltersDokument68 SeitenRectifiers and FiltersMeheli HalderNoch keine Bewertungen
- Sibuyan Island ResiliencyDokument12 SeitenSibuyan Island ResiliencyEndangeredSpeciesNoch keine Bewertungen
- 07 Raction KineticsDokument43 Seiten07 Raction KineticsestefanoveiraNoch keine Bewertungen
- Gautam Samhita CHP 1 CHP 2 CHP 3 ColorDokument22 SeitenGautam Samhita CHP 1 CHP 2 CHP 3 ColorSaptarishisAstrology100% (1)
- Apollo TyresDokument78 SeitenApollo TyresADITYA33% (3)
- Embankment PDFDokument5 SeitenEmbankment PDFTin Win HtutNoch keine Bewertungen
- VT6050 VT6010 QuickGuide ENDokument19 SeitenVT6050 VT6010 QuickGuide ENPriyank KumarNoch keine Bewertungen