Das könnte Ihnen auch gefallen
- Problem-based Approach to Gastroenterology and HepatologyVon EverandProblem-based Approach to Gastroenterology and HepatologyJohn N. PlevrisNoch keine Bewertungen
- Swollen Kidney, (Hydronephrosis) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsVon EverandSwollen Kidney, (Hydronephrosis) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNoch keine Bewertungen
- Reye's SyndromeDokument11 SeitenReye's SyndromeChristine Go100% (1)
- Appendicitis: The Etiology, Hygenic and Dietetic TreatmentVon EverandAppendicitis: The Etiology, Hygenic and Dietetic TreatmentBewertung: 3 von 5 Sternen3/5 (2)
- A Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsVon EverandA Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsNoch keine Bewertungen
- Ventricular Septal Defect, A Simple Guide To The Condition, Treatment And Related ConditionsVon EverandVentricular Septal Defect, A Simple Guide To The Condition, Treatment And Related ConditionsNoch keine Bewertungen
- How Do I Diagnose The Cause of A Cough of Less Than 3 Weeks' Duration?Dokument14 SeitenHow Do I Diagnose The Cause of A Cough of Less Than 3 Weeks' Duration?Sudhir TyagiNoch keine Bewertungen
- Hirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsVon EverandHirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNoch keine Bewertungen
- ICU Scoring Systems A Complete Guide - 2020 EditionVon EverandICU Scoring Systems A Complete Guide - 2020 EditionNoch keine Bewertungen
- A Study of the Lack of Hiv/Aids Awareness Among African American Women: a Leadership Perspective: Awareness That All Cultures Should Know AboutVon EverandA Study of the Lack of Hiv/Aids Awareness Among African American Women: a Leadership Perspective: Awareness That All Cultures Should Know AboutBewertung: 5 von 5 Sternen5/5 (1)
- A Simple Guide to Parathyroid Adenoma, Diagnosis, Treatment and Related ConditionsVon EverandA Simple Guide to Parathyroid Adenoma, Diagnosis, Treatment and Related ConditionsNoch keine Bewertungen
- Patho Physiology of Kawasaki DiseaseDokument2 SeitenPatho Physiology of Kawasaki DiseaseIris CaberteNoch keine Bewertungen
- IM AdconDokument28 SeitenIM AdconCla SantosNoch keine Bewertungen
- Inflamatory Bowel Disease: Dr. Samir IsmailDokument82 SeitenInflamatory Bowel Disease: Dr. Samir IsmailGhadeer EbraheemNoch keine Bewertungen
- EclampsiaDokument56 SeitenEclampsiagalihtrimuninggarNoch keine Bewertungen
- Cardiac NSG DiagnosisDokument5 SeitenCardiac NSG DiagnosisShreyas WalvekarNoch keine Bewertungen
- 08&09 Oral Hypoglycemics-Level 11Dokument48 Seiten08&09 Oral Hypoglycemics-Level 11Usman Ali AkbarNoch keine Bewertungen
- Sree Vasantham Hospital, Salem: 1. Er Protocol For Acute Intoxication (Poisoning)Dokument7 SeitenSree Vasantham Hospital, Salem: 1. Er Protocol For Acute Intoxication (Poisoning)Elango MuthuNoch keine Bewertungen
- Final GIT Case PresentationDokument53 SeitenFinal GIT Case PresentationRovan100% (1)
- Anemia in CKDDokument149 SeitenAnemia in CKDUlises ContrerasNoch keine Bewertungen
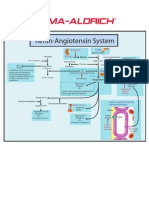
- Renin-Angiotensin SystemDokument1 SeiteRenin-Angiotensin SystemSigma-Aldrich100% (2)
- Post OpDokument6 SeitenPost OpFrinkaWijayaNoch keine Bewertungen
- Kawasaki Disease LectureDokument25 SeitenKawasaki Disease LectureAlif ZainalNoch keine Bewertungen
- Case Protocol Kawasaki DiseaseDokument5 SeitenCase Protocol Kawasaki DiseaseFranz SalazarNoch keine Bewertungen
- Hanson Infectious Diseases - Anamneza I StatusDokument33 SeitenHanson Infectious Diseases - Anamneza I StatusSilvia KesegNoch keine Bewertungen
- Pat 2 Medsurg1Dokument20 SeitenPat 2 Medsurg1api-300849832Noch keine Bewertungen
- C191W003 Control Bleeding and Hypovolemic ShockDokument51 SeitenC191W003 Control Bleeding and Hypovolemic ShockEmad Hussien Haj-AbdullaNoch keine Bewertungen
- Seminar On Hemodynamic Monitoring: BY UMA Iind Year MSC NursingDokument52 SeitenSeminar On Hemodynamic Monitoring: BY UMA Iind Year MSC NursingAyen AlingNoch keine Bewertungen
- Agis Mira Dewi, S.kedDokument35 SeitenAgis Mira Dewi, S.kedAgiish EMdeNoch keine Bewertungen
- Interatitial Lung DiseaseDokument2 SeitenInteratitial Lung DiseaseIsabel CastilloNoch keine Bewertungen
- Chapter 31: Infectious Diseases Garzon Maaks: Burns' Pediatric Primary Care, 7th EditionDokument4 SeitenChapter 31: Infectious Diseases Garzon Maaks: Burns' Pediatric Primary Care, 7th EditionHelen UgochukwuNoch keine Bewertungen
- Transitional Care Case Study-Pulling It All TogetherDokument13 SeitenTransitional Care Case Study-Pulling It All TogethermatthewNoch keine Bewertungen
- Carbuncle, Incision, Drainage, DebridementDokument11 SeitenCarbuncle, Incision, Drainage, DebridementAlvin Germo PasuquinNoch keine Bewertungen
- Standard Treatment of Pyelonephritis in Pregnancy.4Dokument5 SeitenStandard Treatment of Pyelonephritis in Pregnancy.4Maria Fe Esperanza MadambaNoch keine Bewertungen
- Infra-Auricular Mass Case PresDokument8 SeitenInfra-Auricular Mass Case PresEjay Jacob RicamaraNoch keine Bewertungen
- NCP Poststreptococcal GlomerulonephritisDokument12 SeitenNCP Poststreptococcal GlomerulonephritisScarlet ScarletNoch keine Bewertungen
- Normal Ecg ReportDokument27 SeitenNormal Ecg ReportMark DycNoch keine Bewertungen
- Chest Pain.Dokument53 SeitenChest Pain.Shimmering MoonNoch keine Bewertungen
- Iii. Medical ManagementDokument3 SeitenIii. Medical ManagementAlyanna EvangelistaNoch keine Bewertungen
- Rheumatic Heart Disease: Emmanuel Edafe Consultant Interventional Cardiologist, NduDokument36 SeitenRheumatic Heart Disease: Emmanuel Edafe Consultant Interventional Cardiologist, NduPrincewill SeiyefaNoch keine Bewertungen
- Common Ecg Abnormalities PDFDokument2 SeitenCommon Ecg Abnormalities PDFRonNoch keine Bewertungen
- Syphilis ReportDokument76 SeitenSyphilis ReportYogiNoch keine Bewertungen
- Case PCAPDokument2 SeitenCase PCAPNina Anne ParacadNoch keine Bewertungen
- Medical Case of SurgeryDokument7 SeitenMedical Case of SurgerysugisweNoch keine Bewertungen
- Vomiting in Children 2018 PDFDokument19 SeitenVomiting in Children 2018 PDFSamuel DiazNoch keine Bewertungen
- Abdominal TuberculosisDokument12 SeitenAbdominal TuberculosisBimlesh ThakurNoch keine Bewertungen
- 01 Admission Discharge Criteria and TriageDokument5 Seiten01 Admission Discharge Criteria and TriageSuhasani JainNoch keine Bewertungen
- Cerebrovascular Disease (Bleed)Dokument25 SeitenCerebrovascular Disease (Bleed)Margaret Jenaw JenawNoch keine Bewertungen
- Case PresentationDokument20 SeitenCase PresentationMohamad HafyfyNoch keine Bewertungen
- PericarditisDokument29 SeitenPericarditisPavin KumarNoch keine Bewertungen
- Sgarbossa CriteriaDokument5 SeitenSgarbossa Criteriajacknaim7090Noch keine Bewertungen
- Discharge Summary PDFDokument2 SeitenDischarge Summary PDFbalab2311Noch keine Bewertungen
- Essensial Hypertension Pathogenesis and PathophsiologyDokument22 SeitenEssensial Hypertension Pathogenesis and PathophsiologyAmeliana KamaludinNoch keine Bewertungen
- Typhoid FeverDokument38 SeitenTyphoid FeverRonelenePurisimaNoch keine Bewertungen
- Pedia CaseDokument65 SeitenPedia CaseJason MirasolNoch keine Bewertungen
- Gordons Case Pres 1Dokument5 SeitenGordons Case Pres 1JM Asentista0% (1)
- LA Myxoma Case PresentationDokument34 SeitenLA Myxoma Case PresentationWiwik Puji LestariNoch keine Bewertungen
- STS Finals ReviewerDokument21 SeitenSTS Finals ReviewerCoffee BlancaNoch keine Bewertungen
- Daftar Harga e-KATALOG Mei - 2022+linkDokument20 SeitenDaftar Harga e-KATALOG Mei - 2022+linkNovaldo Widodo PutraNoch keine Bewertungen
- L5-6: Tools For Plant Gene Transfer: Promoters Marker Genes - Reporter Genes - Selectable Markers VectorsDokument56 SeitenL5-6: Tools For Plant Gene Transfer: Promoters Marker Genes - Reporter Genes - Selectable Markers VectorsTing Yan LeeNoch keine Bewertungen
- 2018 Calf Immunology and The Role of Vaccinations in Dairy CalvesmvzDokument11 Seiten2018 Calf Immunology and The Role of Vaccinations in Dairy CalvesmvzDavid Julian ClavijoNoch keine Bewertungen
- Letter To Amazon Re: CoronavirusDokument2 SeitenLetter To Amazon Re: CoronavirusSenator Cory Booker100% (4)
- How Do Antibiotics Work - AntibioticsDokument1 SeiteHow Do Antibiotics Work - AntibioticsBrigitte Fani FlorenciaNoch keine Bewertungen
- UntitledDokument9 SeitenUntitledMasar ElfNoch keine Bewertungen
- 5 FOI Webpage Jan 4 2022Dokument119 Seiten5 FOI Webpage Jan 4 2022Luis ricardo Véjar felixNoch keine Bewertungen
- M1 Review On Basic MicrobiologyDokument15 SeitenM1 Review On Basic MicrobiologyPedrosa NardNoch keine Bewertungen
- Determinan Kejadian Demam Berdarah Dengue (DBD) Di Kecamatan Medan Tembung Dian Maya Sari, Sori Muda Sarumpaet, Dan HiswaniDokument17 SeitenDeterminan Kejadian Demam Berdarah Dengue (DBD) Di Kecamatan Medan Tembung Dian Maya Sari, Sori Muda Sarumpaet, Dan HiswaniRyadhianNoch keine Bewertungen
- Script ImmDokument14 SeitenScript ImmVivianNoch keine Bewertungen
- PD 22ND April 2020Dokument32 SeitenPD 22ND April 2020Paul MachariaNoch keine Bewertungen
- PEÑA-RODRIGUEZ2023 Prevalence of Symptoms, Comorbidities, and Reinfections in Individuals Infected With Wild-Type SARS-CoV-2Dokument9 SeitenPEÑA-RODRIGUEZ2023 Prevalence of Symptoms, Comorbidities, and Reinfections in Individuals Infected With Wild-Type SARS-CoV-2Oliver Viera SeguraNoch keine Bewertungen
- Diseases of Passion FruitDokument18 SeitenDiseases of Passion FruitRija Parfait RANDRIANANDRASANANoch keine Bewertungen
- Hsslive Xii Zoology 8 NewDokument5 SeitenHsslive Xii Zoology 8 Newjishnupk135Noch keine Bewertungen
- Antibacterial Drug Discovery To Combat MDR PDFDokument673 SeitenAntibacterial Drug Discovery To Combat MDR PDFTUSHAR DASHNoch keine Bewertungen
- 11.2 Development of ImmunityDokument90 Seiten11.2 Development of ImmunityDaksha yashaNoch keine Bewertungen
- Emerging Infectionus Diseases Sep2012Dokument163 SeitenEmerging Infectionus Diseases Sep2012Suhail Gattan100% (1)
- Immuno ReportDokument14 SeitenImmuno Reportlenny lemoogeNoch keine Bewertungen
- Introduction of Food Processing TechnologyDokument35 SeitenIntroduction of Food Processing TechnologyFriz01Noch keine Bewertungen
- What Is Aids Causing How Long Does HIV Take To Become AIDS Types of HIV Diagnoses Transmission Symptoms Curing (Treatments) Preventing of The DiseaseDokument11 SeitenWhat Is Aids Causing How Long Does HIV Take To Become AIDS Types of HIV Diagnoses Transmission Symptoms Curing (Treatments) Preventing of The DiseaseAsha lakraNoch keine Bewertungen
- Make Table For Morphology!: 1.) Identification: Staphylococcus AureusDokument16 SeitenMake Table For Morphology!: 1.) Identification: Staphylococcus AureusAngel HannahNoch keine Bewertungen
- COVID19 Pandemic: Problems and Reflection in Indonesia: Lecturer: Nina Fatriana, S.PD.,M.PDDokument20 SeitenCOVID19 Pandemic: Problems and Reflection in Indonesia: Lecturer: Nina Fatriana, S.PD.,M.PDGisca Syanitia IINoch keine Bewertungen
- NHMRC - Infection Control Guidelines-Accessible PDFDokument362 SeitenNHMRC - Infection Control Guidelines-Accessible PDFMita Refanita100% (1)
- The 2 Covid-19 Wave in South Africa: Transmissibility & A 501.V2 VariantDokument12 SeitenThe 2 Covid-19 Wave in South Africa: Transmissibility & A 501.V2 VariantBathandwa Malingo100% (6)
- Genital Herpes: The FactsDokument3 SeitenGenital Herpes: The FactstangawangerNoch keine Bewertungen
- Hepatitis Viruses Combination (Blood Borne Pathogens)Dokument51 SeitenHepatitis Viruses Combination (Blood Borne Pathogens)Hosam GomaaNoch keine Bewertungen
- GR 10 - HIV AIDSDokument6 SeitenGR 10 - HIV AIDSNazeera DawoodNoch keine Bewertungen
- Report On Covid 19Dokument9 SeitenReport On Covid 19Valorant PlaysNoch keine Bewertungen
- Homework 3Dokument4 SeitenHomework 3Ashok ThiruvengadamNoch keine Bewertungen