Das könnte Ihnen auch gefallen
- Senior Interns GrandroundsDokument119 SeitenSenior Interns GrandroundsNicko GranadoNoch keine Bewertungen
- SCHIZODokument25 SeitenSCHIZOQuinonez Anna MarieNoch keine Bewertungen
- Protocol - IM DyspneaDokument7 SeitenProtocol - IM DyspneaTrisNoch keine Bewertungen
- Rebira 1Dokument36 SeitenRebira 1Rebira WorkinehNoch keine Bewertungen
- Pediatrics 2 LaboratoryDokument40 SeitenPediatrics 2 LaboratoryAmaetenNoch keine Bewertungen
- OPHTHA Case Report Diabetic RetinopathyDokument51 SeitenOPHTHA Case Report Diabetic RetinopathyJessa MeaNoch keine Bewertungen
- Polycystic Ovarian SyndromeDokument36 SeitenPolycystic Ovarian SyndromeRaras Mayang100% (1)
- (CLINPHAR) 2015 Clinical Practice Guidelines For The Management of Dyslipidemia in The Philippines - ExtractedDokument44 Seiten(CLINPHAR) 2015 Clinical Practice Guidelines For The Management of Dyslipidemia in The Philippines - ExtractedDenise Yanci DemiarNoch keine Bewertungen
- Case Presentation CKDDokument35 SeitenCase Presentation CKDKojo EgyirNoch keine Bewertungen
- Definition:: I. Diagnostic Tests 1. Phases-Pretests Intratests Post Tests 2. Blood Tests - CBCDokument13 SeitenDefinition:: I. Diagnostic Tests 1. Phases-Pretests Intratests Post Tests 2. Blood Tests - CBCKelly Sosa LuyunNoch keine Bewertungen
- Case Presentation OB - GYNDokument14 SeitenCase Presentation OB - GYNRaidah Ayesha RazackNoch keine Bewertungen
- Case Presentation - GASTRODokument46 SeitenCase Presentation - GASTROalidudeNoch keine Bewertungen
- Introduction To HematologyDokument61 SeitenIntroduction To HematologyThis is PonyNoch keine Bewertungen
- Liver Cirrhosis PowerPointDokument12 SeitenLiver Cirrhosis PowerPointFrancis Adrian100% (2)
- Nursing Case Presentation For A Patient With CABG: Subject: Medical Surgical Nursing-IIDokument10 SeitenNursing Case Presentation For A Patient With CABG: Subject: Medical Surgical Nursing-IIanamika sharmaNoch keine Bewertungen
- Case Presentation On Copd: By, Thomas Eipe Pharm D InternDokument32 SeitenCase Presentation On Copd: By, Thomas Eipe Pharm D InternThomas EipeNoch keine Bewertungen
- Multinodular Goitre Case PresentationDokument19 SeitenMultinodular Goitre Case PresentationTamilNoch keine Bewertungen
- Ethical Issues of HIV and AIDS in HealthDokument25 SeitenEthical Issues of HIV and AIDS in HealthSCRIBDISTHEBEASTNoch keine Bewertungen
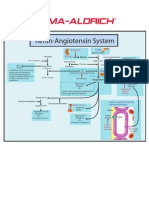
- Renin-Angiotensin SystemDokument1 SeiteRenin-Angiotensin SystemSigma-Aldrich100% (2)
- Nursing Process 3Dokument10 SeitenNursing Process 3Shubhra Sheoran100% (1)
- APPENDICITISDokument69 SeitenAPPENDICITISKim Alvarez100% (1)
- Chemo Side Effects PDFDokument5 SeitenChemo Side Effects PDFImela SariNoch keine Bewertungen
- ProposalDokument22 SeitenProposalbegosewNoch keine Bewertungen
- Testicular CancerDokument24 SeitenTesticular CancerJulianne LeeNoch keine Bewertungen
- HIV:AIDS Determinants and Control of The EpidemicDokument4 SeitenHIV:AIDS Determinants and Control of The EpidemicahiNoch keine Bewertungen
- Nutritional Status of Under-Five Children and Associated FactorsDokument75 SeitenNutritional Status of Under-Five Children and Associated FactorsRoseline Odey100% (2)
- Grand ReportsDokument60 SeitenGrand ReportsfilchibuffNoch keine Bewertungen
- Nephrotic SyndromeeDokument28 SeitenNephrotic SyndromeeRiteka SinghNoch keine Bewertungen
- Diarrheal Disease: DR - Kussia (MD)Dokument34 SeitenDiarrheal Disease: DR - Kussia (MD)Yemata Hailu100% (2)
- Case Report: Kwashiorkor: BY: JAYA DEV (110100465) Supervisor: Dr. Hj. Tiangsa Sembiring, M.Ked (Ped), Sp.A (K)Dokument49 SeitenCase Report: Kwashiorkor: BY: JAYA DEV (110100465) Supervisor: Dr. Hj. Tiangsa Sembiring, M.Ked (Ped), Sp.A (K)Izaac JdevNoch keine Bewertungen
- Cirrhosis Case For PrintingDokument12 SeitenCirrhosis Case For PrintingSean Mercado100% (1)
- NSG6435 Soap3Dokument6 SeitenNSG6435 Soap3Hephzibah BeulahNoch keine Bewertungen
- Cheiloplasty and PalatoplastyDokument41 SeitenCheiloplasty and Palatoplastyapi-325029251Noch keine Bewertungen
- Article On DengueDokument6 SeitenArticle On Dengueاحمد احمدNoch keine Bewertungen
- CM Gastric and Duodenal Contents Examination (Ocfemia, Eliazel G - BSMT4-PLTCI)Dokument53 SeitenCM Gastric and Duodenal Contents Examination (Ocfemia, Eliazel G - BSMT4-PLTCI)eliazel ocfemiaNoch keine Bewertungen
- Pat 2 Medsurg1Dokument20 SeitenPat 2 Medsurg1api-300849832Noch keine Bewertungen
- Chapter 2 - Role of The Government in HealthDokument3 SeitenChapter 2 - Role of The Government in HealthChhavi100% (1)
- Idiopathic Thrombocytopenic PurpuraDokument10 SeitenIdiopathic Thrombocytopenic PurpuramariakolandaNoch keine Bewertungen
- Pediatrics: 2 Case ReportDokument50 SeitenPediatrics: 2 Case ReportSam Raven AndresNoch keine Bewertungen
- Pediatric Urinary Tract Infection Case StudyDokument17 SeitenPediatric Urinary Tract Infection Case StudyKyla Barrera TabungarNoch keine Bewertungen
- Liver Function Test FinalDokument98 SeitenLiver Function Test FinalHussain AzharNoch keine Bewertungen
- Presenter-Dr. Tesita SherryDokument109 SeitenPresenter-Dr. Tesita SherryTesitaNoch keine Bewertungen
- ThalassemiaDokument9 SeitenThalassemiaHanady NaeemNoch keine Bewertungen
- PEDIA - TachypneaDokument12 SeitenPEDIA - TachypneaAlvin Germo PasuquinNoch keine Bewertungen
- PNEUMONIA Case 2 PDFDokument49 SeitenPNEUMONIA Case 2 PDFRed OrangeNoch keine Bewertungen
- Sjogren'S Syndrome: Guided By: Dr. Richa MohanDokument17 SeitenSjogren'S Syndrome: Guided By: Dr. Richa MohanAnkyNoch keine Bewertungen
- CranioplastyDokument2 SeitenCranioplastyLaila munazadNoch keine Bewertungen
- Case Study On IBDDokument41 SeitenCase Study On IBDchampaNoch keine Bewertungen
- HypothyroidismDokument2 SeitenHypothyroidismDanteAndreiNoch keine Bewertungen
- Case Sheet L3Dokument22 SeitenCase Sheet L3Gulfeshan ArshiNoch keine Bewertungen
- Pedia 2017 Case ProtocolDokument14 SeitenPedia 2017 Case ProtocolArjay Amba0% (1)
- Case Presentation - Cholecystitis - DR - RikiDokument14 SeitenCase Presentation - Cholecystitis - DR - RikiLevina AudreyNoch keine Bewertungen
- Drugstudy - OsteoarthritisDokument3 SeitenDrugstudy - OsteoarthritisLizli Loredo100% (1)
- Case Presentation: DR - Anbalagan II ND Year MEMDokument20 SeitenCase Presentation: DR - Anbalagan II ND Year MEMDr mahi sNoch keine Bewertungen
- ANAMEIA PPT BY SandeepDokument32 SeitenANAMEIA PPT BY SandeepSandeep ChakravarthyNoch keine Bewertungen
- Ultrasonography AssignmentDokument5 SeitenUltrasonography AssignmentAkshay VasishtaNoch keine Bewertungen
- Lupus Case PresentationDokument48 SeitenLupus Case PresentationRoscelie KhoNoch keine Bewertungen
- Congenital HypothyroidismDokument50 SeitenCongenital HypothyroidismG VenkateshNoch keine Bewertungen
- OB-Gyn Case Presentation - BicornuateDokument53 SeitenOB-Gyn Case Presentation - BicornuateZari Novela100% (1)
- Case Presentation: Placenta Previa: Crissa Marie D. PinedaDokument42 SeitenCase Presentation: Placenta Previa: Crissa Marie D. PinedaCrissa PinedaNoch keine Bewertungen
- XrayDokument106 SeitenXrayRaine BowNoch keine Bewertungen
- Incisions October December 2011 PDFDokument60 SeitenIncisions October December 2011 PDFRaine BowNoch keine Bewertungen
- Incisions July December 2011 PDFDokument40 SeitenIncisions July December 2011 PDFRaine BowNoch keine Bewertungen
- Incisions July December 2013 PDFDokument40 SeitenIncisions July December 2013 PDFRaine BowNoch keine Bewertungen
- Incisions January June 2014Dokument40 SeitenIncisions January June 2014Raine Bow100% (1)
- Incisions July September 2014Dokument24 SeitenIncisions July September 2014Raine BowNoch keine Bewertungen
- Autoimmune Protocol Ebook 6 19Dokument306 SeitenAutoimmune Protocol Ebook 6 19Hrvoje100% (12)
- Anterolateral Thigh - ALT - Free Flap For Head and Neck ReconstructionDokument12 SeitenAnterolateral Thigh - ALT - Free Flap For Head and Neck ReconstructionАрман ЖуманкуловNoch keine Bewertungen
- Zoology MJ-2 MJ-3Dokument6 SeitenZoology MJ-2 MJ-3vishalbisai07Noch keine Bewertungen
- Grade 6 ScienceDokument10 SeitenGrade 6 ScienceSanjeev NNoch keine Bewertungen
- OjasDokument66 SeitenOjasVineeth Vini100% (1)
- Martini FAP7 ch1Dokument41 SeitenMartini FAP7 ch1Muhammad Na'imNoch keine Bewertungen
- Anatomical Planes, Sections, Terminologies, & Movements: Dr. Syed Wajahat Hasib LecturerDokument25 SeitenAnatomical Planes, Sections, Terminologies, & Movements: Dr. Syed Wajahat Hasib LecturerRameen ZahraNoch keine Bewertungen
- Full Download Test Bank For Holes Essentials of Human Anatomy Physiology 14th Edition Charles Welsh PDF Full ChapterDokument36 SeitenFull Download Test Bank For Holes Essentials of Human Anatomy Physiology 14th Edition Charles Welsh PDF Full Chapterendictsweeta8ce2c100% (17)
- Exs 387 Lab 7Dokument7 SeitenExs 387 Lab 7api-500055972100% (1)
- Human Anatomy and Physiology NotesDokument33 SeitenHuman Anatomy and Physiology NotesFLORLYN VERALNoch keine Bewertungen
- NCPDokument11 SeitenNCPRyan Dela CruzNoch keine Bewertungen
- NCLEX Exam Obstetrical Nursing - Antepartum (50 Items)Dokument13 SeitenNCLEX Exam Obstetrical Nursing - Antepartum (50 Items)Catherine Manalo100% (1)
- Sporogenous TissueDokument4 SeitenSporogenous TissueJewel SajiNoch keine Bewertungen
- Bleeding DisordersDokument4 SeitenBleeding DisordersRitz CelsoNoch keine Bewertungen
- AnaPhy ReviewerDokument2 SeitenAnaPhy ReviewerNashleyah AnayatinNoch keine Bewertungen
- Hematology & Immune SystemDokument81 SeitenHematology & Immune SystemAmanuel Maru100% (1)
- Cytochemistry PrimerDokument2 SeitenCytochemistry PrimerMunish Dogra100% (1)
- Frog DissectionDokument4 SeitenFrog Dissection2110038Noch keine Bewertungen
- Biological Membranes A Biology Questions AQA OCR Edexcel PDFDokument3 SeitenBiological Membranes A Biology Questions AQA OCR Edexcel PDFbekoNoch keine Bewertungen
- Fetal ImagingDokument102 SeitenFetal ImagingDameNoch keine Bewertungen
- Maximum Volume To Which The Lungs Can Be Expanded With The Greatest Possible Inspiratory EffortDokument6 SeitenMaximum Volume To Which The Lungs Can Be Expanded With The Greatest Possible Inspiratory EffortMariz PepitoNoch keine Bewertungen
- Anatomy and Physiology of The SkinDokument30 SeitenAnatomy and Physiology of The SkinNancy VargasNoch keine Bewertungen
- How Do I Carry Out A Resonance Test?Dokument1 SeiteHow Do I Carry Out A Resonance Test?Inayattullah KhamkerNoch keine Bewertungen
- Normal Factor LevelsDokument2 SeitenNormal Factor LevelsY. MadhuriNoch keine Bewertungen
- NeckDokument4 SeitenNeckAttin GamerNoch keine Bewertungen
- Malignant Ovarian TumourDokument42 SeitenMalignant Ovarian TumourJones MarinaNoch keine Bewertungen
- Points and Landmarks - ClassificationDokument28 SeitenPoints and Landmarks - ClassificationMariyamNoch keine Bewertungen
- HSB The Endocrine System Csec NotesDokument4 SeitenHSB The Endocrine System Csec NotesGiaaNoch keine Bewertungen
- Science 10 Quarter 3 Module 3Dokument15 SeitenScience 10 Quarter 3 Module 3Zahra Alexä DavidsonNoch keine Bewertungen
- Wolf Motor Function Test WMFTDokument1 SeiteWolf Motor Function Test WMFTTadeja Hernja Rumpf100% (1)