Das könnte Ihnen auch gefallen
- Acute Stroke Lecture (Fall 2021) 2Dokument47 SeitenAcute Stroke Lecture (Fall 2021) 2shahad alghamdiNoch keine Bewertungen
- Emergent Management of Acute Ischemic Stroke PDF VersionDokument73 SeitenEmergent Management of Acute Ischemic Stroke PDF VersionElizar JarNoch keine Bewertungen
- Nursing Module For Brain StrokeDokument27 SeitenNursing Module For Brain StrokeziadabiakarNoch keine Bewertungen
- Intraserebral Hemoragic: Patofisiologi, Diagnosis, Dan ManajementDokument7 SeitenIntraserebral Hemoragic: Patofisiologi, Diagnosis, Dan ManajementTrigen Rahmat YulisNoch keine Bewertungen
- 60-2017-C5 - Stroke - PlateDokument7 Seiten60-2017-C5 - Stroke - PlateDr. Jayakumar TNoch keine Bewertungen
- Fast Facts for Patients: Thrombotic Thrombocytopenic Purpura: Prompt action saves livesVon EverandFast Facts for Patients: Thrombotic Thrombocytopenic Purpura: Prompt action saves livesNoch keine Bewertungen
- AHA/ASA Guideline - 2007 Guidelines For The Early Management of Adults With Ischemia StrokeDokument8 SeitenAHA/ASA Guideline - 2007 Guidelines For The Early Management of Adults With Ischemia StrokeJadwiga O'GormanNoch keine Bewertungen
- Neurologic EmergenciesDokument11 SeitenNeurologic EmergenciesRoberto López MataNoch keine Bewertungen
- Thrombolisis Dan Trombektomi Pada Stroke AkutDokument48 SeitenThrombolisis Dan Trombektomi Pada Stroke AkutanisNoch keine Bewertungen
- Conversion GateDokument25 SeitenConversion GateThomas HenrryNoch keine Bewertungen
- Acute Stroke Management by Carlos L ChuaDokument61 SeitenAcute Stroke Management by Carlos L ChuaRemaica Hernadez100% (1)
- Activase Rt-PA (Acute Ischemic Stroke)Dokument11 SeitenActivase Rt-PA (Acute Ischemic Stroke)bishoy.youssef.cpiNoch keine Bewertungen
- Extra Acute Ischemic StrokeDokument52 SeitenExtra Acute Ischemic Strokefyqmk4q8pkNoch keine Bewertungen
- ATLS Power Point PDFDokument54 SeitenATLS Power Point PDFRizky LumalessilNoch keine Bewertungen
- Impact of High Sensitivity Troponins For 6nov Cardiac ForumDokument39 SeitenImpact of High Sensitivity Troponins For 6nov Cardiac Forummouna6685Noch keine Bewertungen
- Minggu 3 Dr. Dr. Lisda MANAGEMENT ACUTE ISCHEMIC STROKEDokument47 SeitenMinggu 3 Dr. Dr. Lisda MANAGEMENT ACUTE ISCHEMIC STROKEPaten PisanNoch keine Bewertungen
- Endovascular Treatment For Acute IschemicDokument79 SeitenEndovascular Treatment For Acute IschemicAF KoasNoch keine Bewertungen
- Beyond The Basics of Stroke EvaluationDokument48 SeitenBeyond The Basics of Stroke EvaluationDrGasnasNoch keine Bewertungen
- Enls V 3.0 Protocol Ais Final 0418Dokument25 SeitenEnls V 3.0 Protocol Ais Final 0418Caleb LinNoch keine Bewertungen
- Tissue Plasminogen Activator (tPA) in Acute Ischaemic Stroke: Time For Collegiate Communication and ConsensusDokument4 SeitenTissue Plasminogen Activator (tPA) in Acute Ischaemic Stroke: Time For Collegiate Communication and Consensuskurnia letheNoch keine Bewertungen
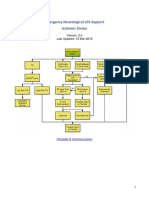
- Emergency Neurological Life Support Ischemic Stroke: Last Updated: 19-Mar-2016Dokument22 SeitenEmergency Neurological Life Support Ischemic Stroke: Last Updated: 19-Mar-2016Aik NoeraNoch keine Bewertungen
- DCV PDFDokument25 SeitenDCV PDFLeyDi CamposanoNoch keine Bewertungen
- Ultra-Early Tranexamic Acid After Subarachnoid Hemorrhage (ULTRA) : Study Protocol For A Randomized Controlled TrialDokument7 SeitenUltra-Early Tranexamic Acid After Subarachnoid Hemorrhage (ULTRA) : Study Protocol For A Randomized Controlled Trialrikadwi20Noch keine Bewertungen
- Update in Stroke ManagementDokument43 SeitenUpdate in Stroke ManagementMuhidin AeNoch keine Bewertungen
- MANAGEMENT ACUTE ISCHEMIC STROKE (Simpo rTPA RSHS) - LisdaDokument63 SeitenMANAGEMENT ACUTE ISCHEMIC STROKE (Simpo rTPA RSHS) - LisdadianNoch keine Bewertungen
- Mutt and JeffDokument8 SeitenMutt and Jeffyoyo1rn100% (2)
- Acute Stroke TreatmentDokument77 SeitenAcute Stroke TreatmentRohitUpadhyayNoch keine Bewertungen
- AtlsDokument32 SeitenAtlsMahesh RajwalNoch keine Bewertungen
- Acute Ischemic Stroke: Nursing's Pivotal RoleDokument34 SeitenAcute Ischemic Stroke: Nursing's Pivotal RoleabolojeenNoch keine Bewertungen
- Thrombolysis Pro & ConsDokument8 SeitenThrombolysis Pro & ConsSofia KusumadewiNoch keine Bewertungen
- TPA Protocol: Stroke in Carefully Selected PersonsDokument4 SeitenTPA Protocol: Stroke in Carefully Selected PersonsJavier Gonzalez, M.D. DABEMNoch keine Bewertungen
- Activating A Stroke Alert - A Neurological Emergency - CE591Dokument7 SeitenActivating A Stroke Alert - A Neurological Emergency - CE591Czar Julius Malasaga100% (1)
- Doppler Atlas SonothrombolysisDokument4 SeitenDoppler Atlas SonothrombolysisdanielNoch keine Bewertungen
- Acute Stroke Guideline January 2017Dokument9 SeitenAcute Stroke Guideline January 2017Nanthini NarsanNoch keine Bewertungen
- Antithrombotic and Thrombolytic Therapy For Ischemic StrokeDokument21 SeitenAntithrombotic and Thrombolytic Therapy For Ischemic StrokeHabibie TifanNoch keine Bewertungen
- Acute Promyelocytic Leukemia Treatment HistoryDokument46 SeitenAcute Promyelocytic Leukemia Treatment HistoryKartthik ShanmugamNoch keine Bewertungen
- Evidence Based Stroke Medicine. Evaluating Treatments For Acute Ischaemic Stroke - What Works and What Doesn't?Dokument32 SeitenEvidence Based Stroke Medicine. Evaluating Treatments For Acute Ischaemic Stroke - What Works and What Doesn't?maluku barat dayaNoch keine Bewertungen
- Prognostic Significance of Troponin T in Acute Myocardial InfarctionDokument6 SeitenPrognostic Significance of Troponin T in Acute Myocardial InfarctionivanNoch keine Bewertungen
- Acute Ischemic Stroke Thrombolysis With Tenecteplase - An Institutional Experience From South India - PMCDokument8 SeitenAcute Ischemic Stroke Thrombolysis With Tenecteplase - An Institutional Experience From South India - PMCviva dialysisNoch keine Bewertungen
- Neurological EmergenciesDokument47 SeitenNeurological EmergenciesStellate Repentance100% (1)
- Antiarrhythmic DrugsVon EverandAntiarrhythmic DrugsAntoni Martínez-RubioNoch keine Bewertungen
- Acute Stroke TreatmentDokument77 SeitenAcute Stroke TreatmentRam PrasadNoch keine Bewertungen
- Stroke and The Emergency DepartmentDokument24 SeitenStroke and The Emergency DepartmentSahuri Sahuri100% (1)
- Dcneo Pituitary IncidentalomaDokument21 SeitenDcneo Pituitary IncidentalomaInes Bilic-ĆurčićNoch keine Bewertungen
- Ying Li 2016Dokument8 SeitenYing Li 2016Bogdan TrandafirNoch keine Bewertungen
- Intravenous Thrombolytic Therapy in Acute Stroke: Frequent Systemic Problems and SolutionsDokument13 SeitenIntravenous Thrombolytic Therapy in Acute Stroke: Frequent Systemic Problems and SolutionsThaer HafiNoch keine Bewertungen
- Acido Tranexamico 2Dokument7 SeitenAcido Tranexamico 2Paola SanchezNoch keine Bewertungen
- Chronic Management of Hypertension After Stroke: The Role of Ambulatory Blood Pressure MonitoringDokument7 SeitenChronic Management of Hypertension After Stroke: The Role of Ambulatory Blood Pressure MonitoringHalbar August KandaNoch keine Bewertungen
- Adj Her 2 SlidesDokument37 SeitenAdj Her 2 SlidesDr. Luis M. Zetina ToacheNoch keine Bewertungen
- Stroke Care and RecoveryDokument4 SeitenStroke Care and RecoverySheenaGuinoCullaNoch keine Bewertungen
- ENLS Acute Ischemic Stroke ProtokolDokument23 SeitenENLS Acute Ischemic Stroke ProtokolFransiskus MikaelNoch keine Bewertungen
- Emergency Neurological Life Support, Protocols.2019.4th EdDokument229 SeitenEmergency Neurological Life Support, Protocols.2019.4th EdMohamad Mostafa100% (1)
- PheochromocytomaDokument30 SeitenPheochromocytomaMirza Yousuf Baig100% (1)
- Phaeochromocytoma - Diagnosis and Management: BackgroundDokument8 SeitenPhaeochromocytoma - Diagnosis and Management: BackgroundaripNoch keine Bewertungen
- Stroke EssentialsDokument44 SeitenStroke Essentialsapi-452244667Noch keine Bewertungen
- Clinical AuditDokument4 SeitenClinical Audithims.qualitymanagerNoch keine Bewertungen
- Essential Guide to Diagnosing and Treating Ischemic StrokeDokument21 SeitenEssential Guide to Diagnosing and Treating Ischemic Strokekuchaibaru90Noch keine Bewertungen
- Intravenus ThrombolysissDokument79 SeitenIntravenus ThrombolysissSilvi VillafuerteNoch keine Bewertungen
- HYPETHYROIDISM NURSING CARE PLANDokument6 SeitenHYPETHYROIDISM NURSING CARE PLANTrisha Joyce MadriagaNoch keine Bewertungen
- Biology 1610 E-Portfolio Assignment PDFDokument4 SeitenBiology 1610 E-Portfolio Assignment PDFapi-437601454Noch keine Bewertungen
- Energy ThumpsDokument3 SeitenEnergy ThumpsTink De NeverlandNoch keine Bewertungen
- Science 4 1st Summative TestDokument2 SeitenScience 4 1st Summative TestEmz FloresNoch keine Bewertungen
- CA Mega Brochure 1090-Rev-B EngDokument6 SeitenCA Mega Brochure 1090-Rev-B EngMuhammad Mahbøøb SadiqNoch keine Bewertungen
- Types of Studies and Research Design PDFDokument5 SeitenTypes of Studies and Research Design PDFPaulina VoicuNoch keine Bewertungen
- USMLE Images For The BoardsDokument297 SeitenUSMLE Images For The BoardsMulham Etki100% (3)
- Steroid Tapering and Supportive Treatment Guidance V1.0 PDFDokument1 SeiteSteroid Tapering and Supportive Treatment Guidance V1.0 PDFNthutagaol TrusNoch keine Bewertungen
- Diasys Katalog 2019 190506 ScreenDokument104 SeitenDiasys Katalog 2019 190506 Screendr-abdullah husseinNoch keine Bewertungen
- Fetal Blood Sampling: 1. PurposeDokument7 SeitenFetal Blood Sampling: 1. PurposeMuathNoch keine Bewertungen
- Amended Modern Pharmacology Syllabus 051218Dokument26 SeitenAmended Modern Pharmacology Syllabus 051218harshad patelNoch keine Bewertungen
- Cardiovascular DisorderDokument6 SeitenCardiovascular DisorderClara De GuzmanNoch keine Bewertungen
- NorovirusDokument3 SeitenNoroviruskolita kamalNoch keine Bewertungen
- Developing Biocompatibility For Medical DevicesDokument30 SeitenDeveloping Biocompatibility For Medical DevicesNagula Naresh100% (1)
- CNS Microbiology MeningitisDokument26 SeitenCNS Microbiology MeningitisSaransh GhimireNoch keine Bewertungen
- Neonatal JaundiceDokument22 SeitenNeonatal JaundiceNivedita Charan100% (1)
- Emergency Medical Technician CPGs PDFDokument121 SeitenEmergency Medical Technician CPGs PDFAnonymous OdW7ev100% (1)
- Adel Elkady Sba PDFDokument290 SeitenAdel Elkady Sba PDFAsh Ame100% (2)
- 5.22 Mission Letter To NC AGDokument4 Seiten5.22 Mission Letter To NC AGMitchell BlackNoch keine Bewertungen
- Peyronies DiseaseDokument6 SeitenPeyronies Diseaseapi-255601700Noch keine Bewertungen
- TCM Patent-Study Guide - FinalDokument9 SeitenTCM Patent-Study Guide - FinalpranajiNoch keine Bewertungen
- ABG Analysis - 5 Steps ROMEDokument2 SeitenABG Analysis - 5 Steps ROMEKschleseNoch keine Bewertungen
- Mechanical AsphyxiaDokument73 SeitenMechanical Asphyxiaapi-61200414Noch keine Bewertungen
- CANINE-Pathophysiology of Organ Failure in Severe Acute Pancreatitis in DogsDokument10 SeitenCANINE-Pathophysiology of Organ Failure in Severe Acute Pancreatitis in Dogstaner_soysurenNoch keine Bewertungen
- Manage High-Risk PregnanciesDokument33 SeitenManage High-Risk PregnanciesDakshayini MbNoch keine Bewertungen
- Manila Tytana CollegesDokument1 SeiteManila Tytana CollegesSkyeNoch keine Bewertungen
- Final Exam Review - Bio 172Dokument21 SeitenFinal Exam Review - Bio 172Erin McElhaney QuirkNoch keine Bewertungen
- CHN 1 Week 13 Lecture MHGAPDokument71 SeitenCHN 1 Week 13 Lecture MHGAPAech EuieNoch keine Bewertungen
- Treating Constipation and Anal Stenosis in a 7-Month-OldDokument35 SeitenTreating Constipation and Anal Stenosis in a 7-Month-OldAbigail CruzNoch keine Bewertungen
- Name_Naw Aung_La Mai Patient Focused ProceduresDokument2 SeitenName_Naw Aung_La Mai Patient Focused ProceduresEileenNoch keine Bewertungen