Das könnte Ihnen auch gefallen
- Reduction, Relocation and Splinting in Emergency Room (RASER)Von EverandReduction, Relocation and Splinting in Emergency Room (RASER)Noch keine Bewertungen
- Trauma MusculoskeletalDokument99 SeitenTrauma MusculoskeletalFatt ZakiNoch keine Bewertungen
- Sprain and Strains, A Simple Guide to the Condition, Treatment and Related DiseasesVon EverandSprain and Strains, A Simple Guide to the Condition, Treatment and Related DiseasesNoch keine Bewertungen
- Complication of FractureDokument79 SeitenComplication of FractureAhmad SyahmiNoch keine Bewertungen
- 11 - Fraktur Dan DislokasiDokument47 Seiten11 - Fraktur Dan DislokasiCarolyn ZhouNoch keine Bewertungen
- Spinal Stenosis And Pinched Nerve A Simple Guide to These conditionsVon EverandSpinal Stenosis And Pinched Nerve A Simple Guide to These conditionsBewertung: 5 von 5 Sternen5/5 (1)
- Medical Surgical Nursing Orthopedic NursingDokument141 SeitenMedical Surgical Nursing Orthopedic Nursingroger92% (12)
- Askep Pada Pasien Dengan Kerusakan Multi SistemDokument76 SeitenAskep Pada Pasien Dengan Kerusakan Multi SistemmeldaiskaNoch keine Bewertungen
- MedSurg Chapter 51 OutlineDokument7 SeitenMedSurg Chapter 51 OutlineJosephine Navarro100% (1)
- Fracture 190706114534Dokument61 SeitenFracture 190706114534Precious BlessingNoch keine Bewertungen
- Surgery - Dychioco - Musculo Skeletal InjuriesDokument79 SeitenSurgery - Dychioco - Musculo Skeletal Injuries3rd yrsNoch keine Bewertungen
- FractureDokument30 SeitenFractureFarida LaksitariniNoch keine Bewertungen
- Pembahasan TTG FrakturDokument48 SeitenPembahasan TTG FrakturErik Ad'perdianNoch keine Bewertungen
- FractureDokument302 SeitenFractureMaryjoy Gabriellee De La CruzNoch keine Bewertungen
- FractureDokument52 SeitenFractureCob CornNoch keine Bewertungen
- Fracture PP Ahmad Aqel 2013Dokument32 SeitenFracture PP Ahmad Aqel 2013ahmadNoch keine Bewertungen
- 10 - Musculoskeletal InjuriesDokument8 Seiten10 - Musculoskeletal InjuriesEastern SamarNoch keine Bewertungen
- Fracture PP Ahmad Aqel 2013Dokument32 SeitenFracture PP Ahmad Aqel 2013aqel605859Noch keine Bewertungen
- Musculoskeletal Trauma RSIJPKDokument41 SeitenMusculoskeletal Trauma RSIJPKPegyNoch keine Bewertungen
- 2 Principles-Of-FracturesDokument94 Seiten2 Principles-Of-Fracturesbyanfqha1Noch keine Bewertungen
- Fracture: Presented By: Ms. Durga Joshi M. SC NursingDokument63 SeitenFracture: Presented By: Ms. Durga Joshi M. SC NursingSanjaya PutraNoch keine Bewertungen
- Fracture RehabilitationDokument43 SeitenFracture Rehabilitationnanahossam12345Noch keine Bewertungen
- Fracture 140717081851 Phpapp02Dokument63 SeitenFracture 140717081851 Phpapp02Jaylord VerazonNoch keine Bewertungen
- Musculoskeletal Disorders FRACTURESDokument10 SeitenMusculoskeletal Disorders FRACTURESرافت العواضيNoch keine Bewertungen
- MS 36Dokument7 SeitenMS 36jefrocNoch keine Bewertungen
- Musculoskeletal Trauma FracturesDokument47 SeitenMusculoskeletal Trauma FracturesLydia Lopz MsnrncdNoch keine Bewertungen
- Fracture and Joint InjuriesDokument32 SeitenFracture and Joint Injuries'putu' AcaaRyaaNoch keine Bewertungen
- Ortho EssentialDokument39 SeitenOrtho EssentialaninuninNoch keine Bewertungen
- Types of FracturesDokument50 SeitenTypes of FracturesMariah Rosette Sison HandomonNoch keine Bewertungen
- Principle of Fractures - Appley (PROF RPT)Dokument62 SeitenPrinciple of Fractures - Appley (PROF RPT)Fuad AbdullahNoch keine Bewertungen
- Basics of FractureDokument12 SeitenBasics of Fracturecimahmudraju100% (2)
- Comprehensive SummaryDokument37 SeitenComprehensive Summaryhrg79qzwc2Noch keine Bewertungen
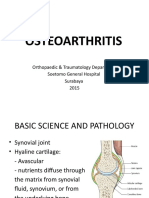
- Osteoarthritis: Orthopaedic & Traumatology Department Soetomo General Hospital Surabaya 2015Dokument31 SeitenOsteoarthritis: Orthopaedic & Traumatology Department Soetomo General Hospital Surabaya 2015internship nganjukNoch keine Bewertungen
- Lahir: Surabaya, 21 April 1970Dokument51 SeitenLahir: Surabaya, 21 April 1970etaNoch keine Bewertungen
- Fractures: Benjamin FarahDokument13 SeitenFractures: Benjamin FarahbennatorNoch keine Bewertungen
- Osteoarthritis of The Knee HKDokument31 SeitenOsteoarthritis of The Knee HKFira Wahidah FirdausNoch keine Bewertungen
- Part 2Dokument8 SeitenPart 2blackforest8Noch keine Bewertungen
- Fractures & DislocationsDokument36 SeitenFractures & DislocationsMozil Fadzil KamarudinNoch keine Bewertungen
- OSTHEOARTHIRITISDokument25 SeitenOSTHEOARTHIRITISOndari gisemba OSINDENoch keine Bewertungen
- Day - 6 RADIOLOGY OF MSKDokument54 SeitenDay - 6 RADIOLOGY OF MSKDewa ayu NarheswariNoch keine Bewertungen
- ActuresDokument41 SeitenActuressylvester GelacNoch keine Bewertungen
- Chapter 65 FracturesDokument43 SeitenChapter 65 FracturesBenjamin SchauerteNoch keine Bewertungen
- Extremity TraumaDokument29 SeitenExtremity TraumaMark CheneyNoch keine Bewertungen
- Bedah Menejemen FrakkturDokument53 SeitenBedah Menejemen FrakkturvitaNoch keine Bewertungen
- Fracturesgoutosteosprain 2Dokument199 SeitenFracturesgoutosteosprain 2Rose Cristille Yeso JocsonNoch keine Bewertungen
- 2 .Bone Fracture ManagementDokument48 Seiten2 .Bone Fracture Managementcctmt5rpphNoch keine Bewertungen
- Medical Rehabilitation in Musculoskeletal Trauma - Prof. Dr. Dr. Angela BM Tulaar SPKFR (K)Dokument41 SeitenMedical Rehabilitation in Musculoskeletal Trauma - Prof. Dr. Dr. Angela BM Tulaar SPKFR (K)YanuarNoch keine Bewertungen
- Complications of FracturesDokument55 SeitenComplications of FracturesMina SamirNoch keine Bewertungen
- Musculoskeletal DisordersDokument42 SeitenMusculoskeletal DisordersSaddichhya TripathiNoch keine Bewertungen
- FIX - Fracture and DislocationDokument80 SeitenFIX - Fracture and DislocationWildan Hilmi AnsoriNoch keine Bewertungen
- Chapter 29Dokument93 SeitenChapter 29api-3743202Noch keine Bewertungen
- Case Study On Normal Vaginal DeliveryDokument40 SeitenCase Study On Normal Vaginal DeliveryPabhat Kumar100% (1)
- Penanganan FrakturDokument78 SeitenPenanganan FrakturelizabethmargarethNoch keine Bewertungen
- Nur Rachmat Lubis: Divisi Orthopaedi Dept Bedah FK UNSRI/ RS Dr. M. Hoesin PalembangDokument38 SeitenNur Rachmat Lubis: Divisi Orthopaedi Dept Bedah FK UNSRI/ RS Dr. M. Hoesin Palembangsoleha09la solehaNoch keine Bewertungen
- 68 DISEASES 2nd Semsester 3rd Year 1 PDFDokument117 Seiten68 DISEASES 2nd Semsester 3rd Year 1 PDFJimlord GarciaNoch keine Bewertungen
- Bahaa Motawea. #. & DislocationsDokument51 SeitenBahaa Motawea. #. & DislocationsFathy AlhallagNoch keine Bewertungen
- 6 Kuliah Radiology of MSKDokument46 Seiten6 Kuliah Radiology of MSKDesak PratiwiNoch keine Bewertungen
- Immobilization and Transport On Patient FractureDokument58 SeitenImmobilization and Transport On Patient FractureDinaNoch keine Bewertungen
- Slide MANTAP BEDAH 2 PDFDokument203 SeitenSlide MANTAP BEDAH 2 PDFIni DiaNoch keine Bewertungen
- Dermatomycosis 2009Dokument29 SeitenDermatomycosis 2009adystiNoch keine Bewertungen
- House Dust Mites DLLDokument32 SeitenHouse Dust Mites DLLadystiNoch keine Bewertungen
- Poisoning DecontaminationDokument14 SeitenPoisoning DecontaminationadystiNoch keine Bewertungen
- Tropical and Infectious Subdivision of Internal Department Medical Faculty of Gadjah Mada University YogyakartaDokument95 SeitenTropical and Infectious Subdivision of Internal Department Medical Faculty of Gadjah Mada University YogyakartaadystiNoch keine Bewertungen
- Venom (Insect Bite, Snake Bite, Dog Bite)Dokument23 SeitenVenom (Insect Bite, Snake Bite, Dog Bite)adystiNoch keine Bewertungen
- Cutaneous Larval MigransDokument24 SeitenCutaneous Larval MigransadystiNoch keine Bewertungen
- Erythrosquamous Diseases / Papulosquamous DiseasesDokument38 SeitenErythrosquamous Diseases / Papulosquamous DiseasesadystiNoch keine Bewertungen
- 10 Tahapan Pidi - 16042016Dokument1 Seite10 Tahapan Pidi - 16042016adystiNoch keine Bewertungen
- VTE Prophylaxis in The Hospital: Johan KurniandaDokument35 SeitenVTE Prophylaxis in The Hospital: Johan KurniandaadystiNoch keine Bewertungen
- Tobacco LectureDokument36 SeitenTobacco LecturesenoNoch keine Bewertungen
- Peripheral Arterial Occlusive DiseaseDokument49 SeitenPeripheral Arterial Occlusive DiseaseadystiNoch keine Bewertungen
- Peripheral Arterial Occlusive DiseaseDokument43 SeitenPeripheral Arterial Occlusive DiseaseadystiNoch keine Bewertungen
- Peripheral Arterial Occlusive DiseaseDokument43 SeitenPeripheral Arterial Occlusive DiseaseadystiNoch keine Bewertungen
- Amblyopia Inter Blok 22Dokument30 SeitenAmblyopia Inter Blok 22adystiNoch keine Bewertungen
- Fever in Children 2010Dokument27 SeitenFever in Children 2010adystiNoch keine Bewertungen
- Vasculer Imaging 2012 PDFDokument72 SeitenVasculer Imaging 2012 PDFadystiNoch keine Bewertungen
- Drug AllergyDokument61 SeitenDrug Allergyadysti100% (1)
- AFP - Blok 3.4. IndoDokument36 SeitenAFP - Blok 3.4. IndoadystiNoch keine Bewertungen
- Immunization: Mei Neni S Pediatric Dept. Faculty of Medicine, Gadjah Mada UniversityDokument35 SeitenImmunization: Mei Neni S Pediatric Dept. Faculty of Medicine, Gadjah Mada UniversityadystiNoch keine Bewertungen
- Dermatitis & Urticaria: Department of Dermato Venereology Faculty of Medicine Gadjah Mada UniversityDokument34 SeitenDermatitis & Urticaria: Department of Dermato Venereology Faculty of Medicine Gadjah Mada UniversityadystiNoch keine Bewertungen
- Genito Urinary Problems in Children: Bagian Ilmu Kesehatan Kulit & Kelamin Fakultas Kedokteran UGM YogyakartaDokument78 SeitenGenito Urinary Problems in Children: Bagian Ilmu Kesehatan Kulit & Kelamin Fakultas Kedokteran UGM YogyakartaadystiNoch keine Bewertungen
- 1 Generation: Cefalexin Cefradin Cefadroxil Cefachlor Yes Yes Yes Yes YesDokument67 Seiten1 Generation: Cefalexin Cefradin Cefadroxil Cefachlor Yes Yes Yes Yes YesadystiNoch keine Bewertungen
- Vaccine Preventable Diseases (VPDS) : Ida Safitri Laksono Dept of Child Health Infectious Disease Sub DivisionDokument26 SeitenVaccine Preventable Diseases (VPDS) : Ida Safitri Laksono Dept of Child Health Infectious Disease Sub DivisionadystiNoch keine Bewertungen
- Imunol InfeksiDokument26 SeitenImunol InfeksiadystiNoch keine Bewertungen
- BasicImmunol PDFDokument56 SeitenBasicImmunol PDFadystiNoch keine Bewertungen
- Aging and Endocrine DisordersDokument23 SeitenAging and Endocrine DisordersadystiNoch keine Bewertungen
- Patient Autonomy: Competent and Incompetent Patient and Research Participant To ConsentDokument27 SeitenPatient Autonomy: Competent and Incompetent Patient and Research Participant To ConsentadystiNoch keine Bewertungen
- Alrg 10 PDFDokument59 SeitenAlrg 10 PDFadystiNoch keine Bewertungen
- Eritro ADokument40 SeitenEritro AadystiNoch keine Bewertungen
- Oportunistic in ElderlyDokument19 SeitenOportunistic in ElderlyadystiNoch keine Bewertungen
- Postoperative Care: Postoperative Note and OrdersDokument4 SeitenPostoperative Care: Postoperative Note and OrdersAhmedNoch keine Bewertungen
- Lung AbscessDokument2 SeitenLung Abscessoxidalaj100% (1)
- Cytopathology of Infectious DiseasesDokument404 SeitenCytopathology of Infectious DiseasesSultan AlexandruNoch keine Bewertungen
- Legal and Ethical Issues-ModifiedDokument29 SeitenLegal and Ethical Issues-Modifiedmonir61100% (1)
- Pancreatic MassDokument124 SeitenPancreatic MassKMNoch keine Bewertungen
- Ug NotesDokument538 SeitenUg NotesSteven IStudy SmithNoch keine Bewertungen
- ACLS DrugDokument7 SeitenACLS DrugPhongsatorn Thunin100% (1)
- As Far As Possible - en ISO 14971Dokument19 SeitenAs Far As Possible - en ISO 14971Kanwal Jit Singh100% (1)
- Tracheostomy Care Reflective EssayDokument2 SeitenTracheostomy Care Reflective EssayAnjae Gariando100% (3)
- Efficacy of Nerve Flossing Technique On Improving Sciatic Nerve Function in Patients With Sciatica - A Randomized Controlled TrialDokument10 SeitenEfficacy of Nerve Flossing Technique On Improving Sciatic Nerve Function in Patients With Sciatica - A Randomized Controlled Trialsphadungkit100% (1)
- Marijuana: A Modern MedicineDokument2 SeitenMarijuana: A Modern MedicineJericho AbiasNoch keine Bewertungen
- Essential Elements of Clinical TrialDokument39 SeitenEssential Elements of Clinical TrialmisganaNoch keine Bewertungen
- Drug Study 8Dokument3 SeitenDrug Study 8Vicky RoqueNoch keine Bewertungen
- Carrie Frechette, LVN: ContactDokument2 SeitenCarrie Frechette, LVN: ContactCARRIE FRECHETTENoch keine Bewertungen
- Green Back TanjyDokument20 SeitenGreen Back TanjymymicroNoch keine Bewertungen
- Coping Mechanisms and Ego DefenseDokument25 SeitenCoping Mechanisms and Ego DefensePrakash16100% (1)
- Posterior Capsular CalcificationDokument4 SeitenPosterior Capsular CalcificationNurulSyaidahNoch keine Bewertungen
- Acute Limb Ischemic: Titien Buniyati Ali Aspar MappahyaDokument40 SeitenAcute Limb Ischemic: Titien Buniyati Ali Aspar MappahyaNurhasanah WahabNoch keine Bewertungen
- Pub104 WorkbookDokument16 SeitenPub104 Workbooksyang9Noch keine Bewertungen
- Sports Injury Assessment PDFDokument43 SeitenSports Injury Assessment PDFVishal Parnerkar50% (2)
- CTNeoBC Pooled AnalysisDokument9 SeitenCTNeoBC Pooled AnalysistabaresgonzaloNoch keine Bewertungen
- Department of Oral Periodontology: Topic: Free Gingival GraftDokument1 SeiteDepartment of Oral Periodontology: Topic: Free Gingival GraftTenzin WangyalNoch keine Bewertungen
- Basic Life Support (BLS) Training Course: FeaturesDokument1 SeiteBasic Life Support (BLS) Training Course: FeaturesSheryl Fuentes De GuzmanNoch keine Bewertungen
- 4.management of Vertical Discrepancies (2) 2Dokument97 Seiten4.management of Vertical Discrepancies (2) 2Arun Joy100% (2)
- Fluoroquinolone-Associated Tendon-Rupture: A Summary of Reports in The Food and Drug Administration's Adverse Event Reporting SystemDokument9 SeitenFluoroquinolone-Associated Tendon-Rupture: A Summary of Reports in The Food and Drug Administration's Adverse Event Reporting SystemMadalinaMadaNoch keine Bewertungen
- Neoplasia ExamDokument9 SeitenNeoplasia ExamYheng Gaosaii100% (1)
- IHOP - 09.13.28 - Surgical Counts PDFDokument3 SeitenIHOP - 09.13.28 - Surgical Counts PDFO.r. CadzNoch keine Bewertungen
- Medical Claim Form - FLEX StaffDokument1 SeiteMedical Claim Form - FLEX StaffHerawaty Syaiful GusmentaNoch keine Bewertungen
- Pre Employment Occupational Health FormDokument7 SeitenPre Employment Occupational Health Formlinks2309Noch keine Bewertungen
- Annotated BibliographyDokument2 SeitenAnnotated Bibliographyapi-237172063Noch keine Bewertungen