Das könnte Ihnen auch gefallen
- NSAIDs, DMARDs & Antigout1Dokument69 SeitenNSAIDs, DMARDs & Antigout1Melissa SalayogNoch keine Bewertungen
- Antiinflammatory Drugs: Toya AriawanDokument27 SeitenAntiinflammatory Drugs: Toya Ariawanlast100% (1)
- Nsaids Nonsteroidal Anti-Inflammatory Drugs: Maher Khdour Msc. Phd. Clinical PharmacyDokument65 SeitenNsaids Nonsteroidal Anti-Inflammatory Drugs: Maher Khdour Msc. Phd. Clinical PharmacyYousef JafarNoch keine Bewertungen
- Autacoids For Med.Dokument140 SeitenAutacoids For Med.Feysal AhmedNoch keine Bewertungen
- AntiemeticsDokument10 SeitenAntiemeticsnk999999100% (1)
- AnemiaDokument13 SeitenAnemiaharizmnNoch keine Bewertungen
- Lecture 1 PDFDokument75 SeitenLecture 1 PDFBasil Elbushra Ahmed DomiNoch keine Bewertungen
- Premedicantdrugs1 170216071329Dokument49 SeitenPremedicantdrugs1 170216071329Sagar BhardwajNoch keine Bewertungen
- 2&3-Pharmacology of Drugs Used in Bronchial Asthma & COPDDokument58 Seiten2&3-Pharmacology of Drugs Used in Bronchial Asthma & COPDKishan SethNoch keine Bewertungen
- TB TreatmentDokument58 SeitenTB TreatmentNdayisaba CorneilleNoch keine Bewertungen
- Antibiotics 9Dokument11 SeitenAntibiotics 9Beth Morales100% (1)
- By: DR Eyad Talal: Moderator: DR I - QudaisatDokument55 SeitenBy: DR Eyad Talal: Moderator: DR I - QudaisatEyad AbdeljawadNoch keine Bewertungen
- Community Acquired PneumoniaDokument37 SeitenCommunity Acquired PneumoniaJoean CabarlocNoch keine Bewertungen
- Preanesthetic Medication JasminaDokument44 SeitenPreanesthetic Medication Jasminaanjali sNoch keine Bewertungen
- AtaxiaDokument8 SeitenAtaxiaDivya Gupta0% (1)
- Respi DrugsDokument36 SeitenRespi DrugsLady Mae RamosNoch keine Bewertungen
- 1a..antimicrobials IntroductionDokument84 Seiten1a..antimicrobials IntroductionAnonymous RlDDdTAsKJNoch keine Bewertungen
- Mechanism of Action For Each Class of AntiDokument146 SeitenMechanism of Action For Each Class of AntiReynaldo RiveraNoch keine Bewertungen
- Adverse Drug EffectsDokument66 SeitenAdverse Drug EffectsSuba Ranjana BalaNoch keine Bewertungen
- Uworld JournalDokument3 SeitenUworld JournalJayNoch keine Bewertungen
- AntibioticsDokument84 SeitenAntibioticsNandini GulurNoch keine Bewertungen
- Cerebral Palsy 08.04.15 LectureDokument25 SeitenCerebral Palsy 08.04.15 LectureEmmanuel MukukaNoch keine Bewertungen
- AntibioticsDokument30 SeitenAntibioticsRoza RahbeniNoch keine Bewertungen
- Brain InfectionDokument61 SeitenBrain Infectionmanisha paikarayNoch keine Bewertungen
- Drugs For Heart Failure: Drugs Catego Ry Drug Function Adverse Effect NoteDokument2 SeitenDrugs For Heart Failure: Drugs Catego Ry Drug Function Adverse Effect NoteyukariNoch keine Bewertungen
- Pharmacology of Drugs Used in Bronchial Asthma & COPDDokument84 SeitenPharmacology of Drugs Used in Bronchial Asthma & COPDdfngjlnNoch keine Bewertungen
- KMU Blood DisorderDokument43 SeitenKMU Blood DisorderSHAFIQNoch keine Bewertungen
- Drugs Used in Hypertension: Dr. R. PilvinieneDokument33 SeitenDrugs Used in Hypertension: Dr. R. PilvinieneNewteNoch keine Bewertungen
- Approach To Comatose Child: DR G.VenkateshDokument83 SeitenApproach To Comatose Child: DR G.VenkateshG VenkateshNoch keine Bewertungen
- Asthma: Pio T. Esguerra II, MD, FPCP, FPCCP Pulmonary & Critical Care FEU-NRMF Medical CenterDokument98 SeitenAsthma: Pio T. Esguerra II, MD, FPCP, FPCCP Pulmonary & Critical Care FEU-NRMF Medical CenteryayayanizaNoch keine Bewertungen
- AnxietyDokument5 SeitenAnxietyJohn HolmesNoch keine Bewertungen
- Anemia in ChildrenDokument4 SeitenAnemia in ChildrenTeslim Raji100% (1)
- Drugs Used For GlaucomaDokument40 SeitenDrugs Used For GlaucomaAgust SalimNoch keine Bewertungen
- Adrenergic AntagonistsDokument6 SeitenAdrenergic Antagonistsfiena92100% (2)
- Review Notes For Diabetes MellitusDokument8 SeitenReview Notes For Diabetes MellitusEditha LucasNoch keine Bewertungen
- Mishba +pharmacology + Tapan ShahDokument232 SeitenMishba +pharmacology + Tapan ShahRaushan BlakeNoch keine Bewertungen
- Sleep Apnoea - Prof - DR K.K.PDokument44 SeitenSleep Apnoea - Prof - DR K.K.PjialeongNoch keine Bewertungen
- Adverse Drug Reactions (ADRS)Dokument24 SeitenAdverse Drug Reactions (ADRS)ANAM IQBALNoch keine Bewertungen
- Approach To Unconscious PatientDokument23 SeitenApproach To Unconscious Patienttantw880% (1)
- Questions For OSCE Exam - Model AnswersDokument9 SeitenQuestions For OSCE Exam - Model AnswersFarah FarahNoch keine Bewertungen
- Cholinergic Anticholinergic DrugsDokument60 SeitenCholinergic Anticholinergic DrugsMD. RASEL MAHMUD MIMNoch keine Bewertungen
- Cholinergic DrugsDokument6 SeitenCholinergic Drugssunshine151Noch keine Bewertungen
- Gastrointestinal Infections Shigellosis InfectionsDokument6 SeitenGastrointestinal Infections Shigellosis InfectionsNishita ChandNoch keine Bewertungen
- 7 - Cholinomimetic DrugsDokument50 Seiten7 - Cholinomimetic DrugslalitrajindoliaNoch keine Bewertungen
- Medical Boards Step 2 Made Ridiculously Simple (Medicalstudyzone - Com)Dokument377 SeitenMedical Boards Step 2 Made Ridiculously Simple (Medicalstudyzone - Com)Benyamin KhalevNoch keine Bewertungen
- Mu 002Dokument10 SeitenMu 002chandanNoch keine Bewertungen
- Adrenergic AgonistsDokument40 SeitenAdrenergic AgonistsBenedict Brashi100% (1)
- Anticholinergic MnemonicDokument1 SeiteAnticholinergic Mnemonictainah07Noch keine Bewertungen
- Drug AllergyDokument61 SeitenDrug Allergyadysti100% (1)
- A Summary of The Chemical Mediators Involve in The Acute Inflammatory Response Is Shown in The Table BelowDokument30 SeitenA Summary of The Chemical Mediators Involve in The Acute Inflammatory Response Is Shown in The Table Belowinny100% (1)
- PharmacogeneticsDokument3 SeitenPharmacogeneticsPardeep Sony100% (1)
- Antiviral Drugs Acting Against RNA Viruses: HIV: PHRM 412Dokument57 SeitenAntiviral Drugs Acting Against RNA Viruses: HIV: PHRM 412Apurba Sarker ApuNoch keine Bewertungen
- Complement SystemDokument21 SeitenComplement SystemEl FatihNoch keine Bewertungen
- ANTICHOLINERGICDokument4 SeitenANTICHOLINERGICSUTHANNoch keine Bewertungen
- AntihistaminesDokument66 SeitenAntihistaminesAfif Bastian100% (1)
- Cholinergic Drug MnemonicsDokument1 SeiteCholinergic Drug Mnemonicssunshine151100% (1)
- ConstipationDokument80 SeitenConstipationVilasineeAriHaraKumarNoch keine Bewertungen
- Drug Toxicity and PoisoningDokument12 SeitenDrug Toxicity and PoisoningPAULA MARIE MERCADO LLIDONoch keine Bewertungen
- 3rd Year MBBS - NEWDokument4 Seiten3rd Year MBBS - NEWDR AbidNoch keine Bewertungen
- CorticoDokument5 SeitenCorticoDR AbidNoch keine Bewertungen
- Near Expiray-21Dokument1 SeiteNear Expiray-21DR AbidNoch keine Bewertungen
- Update BillDokument1 SeiteUpdate BillDR AbidNoch keine Bewertungen
- Medicine in Insaf CardDokument1 SeiteMedicine in Insaf CardDR AbidNoch keine Bewertungen
- Camp Patient DetailDokument2 SeitenCamp Patient DetailDR AbidNoch keine Bewertungen
- Instapdf - in Pharmacology and Toxicology Mcqs With Answers 419 PDFDokument12 SeitenInstapdf - in Pharmacology and Toxicology Mcqs With Answers 419 PDFDR AbidNoch keine Bewertungen
- SodapdfDokument5 SeitenSodapdfDR AbidNoch keine Bewertungen
- Available Medicine at PharmacyDokument4 SeitenAvailable Medicine at PharmacyDR AbidNoch keine Bewertungen
- Pre Anesthetics Local AnestheticsDokument45 SeitenPre Anesthetics Local AnestheticsDR AbidNoch keine Bewertungen
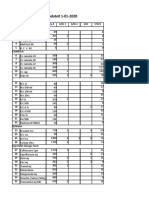
- Items Kept Temp Below 25Dokument1 SeiteItems Kept Temp Below 25DR AbidNoch keine Bewertungen
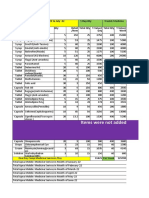
- Apna Moblie Service Year 22 Medicine ExpensiveDokument8 SeitenApna Moblie Service Year 22 Medicine ExpensiveDR AbidNoch keine Bewertungen
- Anti HypertensiveDokument4 SeitenAnti HypertensiveDR AbidNoch keine Bewertungen
- Surgical PT Data 22Dokument4 SeitenSurgical PT Data 22DR AbidNoch keine Bewertungen
- Camp Patient DetailDokument2 SeitenCamp Patient DetailDR AbidNoch keine Bewertungen
- Emergency KITS MedicineDokument3 SeitenEmergency KITS MedicineDR AbidNoch keine Bewertungen
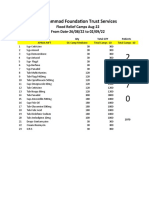
- MFT-Flood ServicesDokument1 SeiteMFT-Flood ServicesDR AbidNoch keine Bewertungen
- No of Patient Admitted Yearly Report of Packages in Gynae WardDokument1 SeiteNo of Patient Admitted Yearly Report of Packages in Gynae WardDR AbidNoch keine Bewertungen
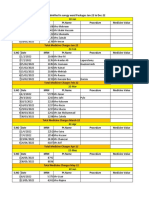
- Camp Daily SheetDokument688 SeitenCamp Daily SheetDR AbidNoch keine Bewertungen
- Potassium SparingDokument22 SeitenPotassium SparingDR AbidNoch keine Bewertungen
- 3rdyear Mbbs-Pharma Assignments-28th Week ResultDokument4 Seiten3rdyear Mbbs-Pharma Assignments-28th Week ResultDR AbidNoch keine Bewertungen
- SodapdfDokument14 SeitenSodapdfDR AbidNoch keine Bewertungen
- NMJ Full OspeDokument2 SeitenNMJ Full OspeDR AbidNoch keine Bewertungen
- MCQ Points of PharmacologyDokument12 SeitenMCQ Points of PharmacologyDR AbidNoch keine Bewertungen
- PG Full OseDokument2 SeitenPG Full OseDR AbidNoch keine Bewertungen
- Regarding Β Blockers: Liaquat University Of Medical & Health Sciences JamshoroDokument2 SeitenRegarding Β Blockers: Liaquat University Of Medical & Health Sciences JamshoroDR AbidNoch keine Bewertungen
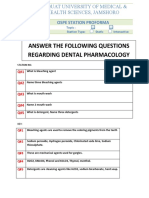
- Dental Pharmacology: Liaquat University of Medical & Health Sciences JamshoroDokument2 SeitenDental Pharmacology: Liaquat University of Medical & Health Sciences JamshoroDR AbidNoch keine Bewertungen
- Insaf Card Medicine Record Jan-22 To July-22Dokument14 SeitenInsaf Card Medicine Record Jan-22 To July-22DR AbidNoch keine Bewertungen
- Mouth Ulcer - OSPEDokument1 SeiteMouth Ulcer - OSPEDR AbidNoch keine Bewertungen
- Dental pharOSPEDokument1 SeiteDental pharOSPEDR AbidNoch keine Bewertungen
- Anti Inflamatory Drugs AINSDokument39 SeitenAnti Inflamatory Drugs AINSEl FaroukNoch keine Bewertungen
- NSAIDS ComparisonDokument60 SeitenNSAIDS ComparisonsillymajorNoch keine Bewertungen
- Nsaids and DmardsDokument59 SeitenNsaids and DmardsBaidawu Weso-amo IbrahimNoch keine Bewertungen
- Ultimate Pre-Reg BNF NotesDokument29 SeitenUltimate Pre-Reg BNF NotesBob100% (7)
- Resep IbuprofenDokument8 SeitenResep Ibuprofen27. SYAHRIN AZRIL IZULKHAQUENoch keine Bewertungen
- Analgesic and Antiinflammatory Activity-2Dokument12 SeitenAnalgesic and Antiinflammatory Activity-2Samantha Vhiel VicenteNoch keine Bewertungen
- Lec9 د ذو الفقارDokument4 SeitenLec9 د ذو الفقارMohammed JaberNoch keine Bewertungen
- Interaksi Obat BukuDokument147 SeitenInteraksi Obat BukuSandhy TampubolonNoch keine Bewertungen
- Nonsteroidal Anti-Inflamatory DrugsDokument4 SeitenNonsteroidal Anti-Inflamatory DrugsYogi drNoch keine Bewertungen
- Utero Re Laks AnDokument8 SeitenUtero Re Laks AnInce NurfiantyNoch keine Bewertungen
- Drugs in The Neonatal Unit: 1 Julia PettyDokument5 SeitenDrugs in The Neonatal Unit: 1 Julia PettyMarjoNoch keine Bewertungen
- Oxytocics and TocolyticsDokument46 SeitenOxytocics and TocolyticsAmanuel Maru50% (2)
- Anti-Inflammatory Activity On Hibiscus Sabdariffa SeedsDokument5 SeitenAnti-Inflammatory Activity On Hibiscus Sabdariffa SeedsDr. Ramadevi DevarakondaNoch keine Bewertungen
- Hot Topics of PEDIATRICS Updated 4th Edition 2016Dokument576 SeitenHot Topics of PEDIATRICS Updated 4th Edition 2016Firas AnayaNoch keine Bewertungen
- APGODokument49 SeitenAPGOiamdonutNoch keine Bewertungen
- ArbutinDokument38 SeitenArbutinWajah IndahNoch keine Bewertungen
- Mecanismo de Acción Del AcetaminofénDokument9 SeitenMecanismo de Acción Del AcetaminofénCero Excusas SA de C.VNoch keine Bewertungen
- NsaidDokument17 SeitenNsaidnoviasinataNoch keine Bewertungen
- Effects of Ethanol Extract of Cissus Quadrangularis OnDokument6 SeitenEffects of Ethanol Extract of Cissus Quadrangularis OnمحمدأميندماجNoch keine Bewertungen
- Comprehensive Geriatric AssessmentDokument75 SeitenComprehensive Geriatric AssessmentBodat BodatsNoch keine Bewertungen
- Ipomoea Aquatica FDokument7 SeitenIpomoea Aquatica FTyasFsbaNoch keine Bewertungen
- Analgesic & Anti Inflammatory DrugsDokument39 SeitenAnalgesic & Anti Inflammatory DrugschicagomdNoch keine Bewertungen
- The Effect of Swietenia Mahogani (Mahogany) Seed Extract On Indomethacin-Induced Gastric Ulcers in Female Sprague-Dawley Rats.Dokument13 SeitenThe Effect of Swietenia Mahogani (Mahogany) Seed Extract On Indomethacin-Induced Gastric Ulcers in Female Sprague-Dawley Rats.Gregory Kalona100% (2)
- PrescriptionDokument16 SeitenPrescriptionRyan KadavilNoch keine Bewertungen
- Nervous System Drugs: Drugs For Pain Management: Non-Narcotic and Narcotic AnalgesicsDokument29 SeitenNervous System Drugs: Drugs For Pain Management: Non-Narcotic and Narcotic AnalgesicsJon Corpuz AggasidNoch keine Bewertungen
- Clinical Guidelines in Neonatology 1st EditionDokument958 SeitenClinical Guidelines in Neonatology 1st EditionGaby Rivera0% (1)
- Arjuna in AyurvedaDokument6 SeitenArjuna in AyurvedaugoNoch keine Bewertungen
- Poly Hydro MN IosDokument21 SeitenPoly Hydro MN IosAsimNoch keine Bewertungen
- Role of Drugs in Orthodontics / Orthodontic Courses by Indian Dental AcademyDokument239 SeitenRole of Drugs in Orthodontics / Orthodontic Courses by Indian Dental Academyindian dental academyNoch keine Bewertungen
- 3329 3337 PDFDokument10 Seiten3329 3337 PDFFarid RakhmanNoch keine Bewertungen