Das könnte Ihnen auch gefallen
- The Use of Temporoparietal Fascia Flap For Surgical Treatment of Traumatic Auricle DefectsDokument5 SeitenThe Use of Temporoparietal Fascia Flap For Surgical Treatment of Traumatic Auricle Defectslia indria watiNoch keine Bewertungen
- Articol PMFDokument6 SeitenArticol PMFclaudia lupuNoch keine Bewertungen
- EDJ - Volume 62 - Issue Issue 1 - January (Oral Surgery) - Pages 955-958Dokument4 SeitenEDJ - Volume 62 - Issue Issue 1 - January (Oral Surgery) - Pages 955-958Mohammed FaroukNoch keine Bewertungen
- Ijomi 15 415Dokument4 SeitenIjomi 15 415Bagis Emre GulNoch keine Bewertungen
- Archotol 1983 00800170041011Dokument3 SeitenArchotol 1983 00800170041011abhishekjha0082Noch keine Bewertungen
- International Journal of Health Sciences and ResearchDokument6 SeitenInternational Journal of Health Sciences and ResearchDentist HereNoch keine Bewertungen
- Non-Bone Graft Associated Regenerative Periodontal TherapyDokument80 SeitenNon-Bone Graft Associated Regenerative Periodontal TherapyGorremuchu Srinivas0% (1)
- Sinus Lift ChenDokument10 SeitenSinus Lift ChenCarlos Frederico Nunes PavãoNoch keine Bewertungen
- Vertical Platysma Myocutaneous Flap That Sacrifices The Facial Artery and VeinDokument6 SeitenVertical Platysma Myocutaneous Flap That Sacrifices The Facial Artery and VeinAnkita GuravNoch keine Bewertungen
- Flap-Free Treatment of An Oroantral Communication With Platelet-Rich (Autosaved)Dokument35 SeitenFlap-Free Treatment of An Oroantral Communication With Platelet-Rich (Autosaved)Vishnu PreethamNoch keine Bewertungen
- Full-Thickness Skin Grafting in Nasal ReconstructionDokument6 SeitenFull-Thickness Skin Grafting in Nasal ReconstructionMuhammad FaizalNoch keine Bewertungen
- TurbinoplastyDokument7 SeitenTurbinoplastyNeena GuptaNoch keine Bewertungen
- JC TopicDokument6 SeitenJC Topicवाधूलं कण्णन् कुमारस्वामिNoch keine Bewertungen
- Total Face, Eyelids, Ears, Scalp, and Skeletal TransplantDokument15 SeitenTotal Face, Eyelids, Ears, Scalp, and Skeletal TransplantPeter Paul PascualNoch keine Bewertungen
- Surgical Incisions Balancing Surgical and Cosmetic Outcomes in Head and Neck OncosurgeryDokument4 SeitenSurgical Incisions Balancing Surgical and Cosmetic Outcomes in Head and Neck OncosurgeryDwarika Prasad BajgaiNoch keine Bewertungen
- Acfs 2019 00668 PDFDokument4 SeitenAcfs 2019 00668 PDFChandra BudiNoch keine Bewertungen
- 1482 5294 1 PBDokument5 Seiten1482 5294 1 PBNikola PachoovNoch keine Bewertungen
- Whale's Tail TechniqueDokument32 SeitenWhale's Tail Techniquevijeta vyasNoch keine Bewertungen
- пожтяжка губ 4Dokument6 Seitenпожтяжка губ 4Alexey SorokinNoch keine Bewertungen
- The Use of PRF in Covering Exposed ImplantDokument6 SeitenThe Use of PRF in Covering Exposed ImplantMohammad AkheelNoch keine Bewertungen
- Treatment of An Intrabony Defect CombinedDokument29 SeitenTreatment of An Intrabony Defect CombinedDR.AMITHBABU.C.BNoch keine Bewertungen
- Chotipanich 2018Dokument5 SeitenChotipanich 2018abhishekjha0082Noch keine Bewertungen
- Reconstruction of Periorbital Defects Using A Modified Tenzel FlapDokument6 SeitenReconstruction of Periorbital Defects Using A Modified Tenzel FlapChandra BudiNoch keine Bewertungen
- The Anatomical Subunit Approach To Managing TessieDokument7 SeitenThe Anatomical Subunit Approach To Managing TessieVictoriaNoch keine Bewertungen
- Parotidectomy For Benign Parotid Tumors: An Aesthetic ApproachDokument6 SeitenParotidectomy For Benign Parotid Tumors: An Aesthetic ApproachamelNoch keine Bewertungen
- Face Lift PaperDokument1 SeiteFace Lift PaperHisham Seify MD,PhDNoch keine Bewertungen
- The Palatal Advanced Flap: A Pedicle Flap For Primary Coverage of Immediately Placed ImplantsDokument7 SeitenThe Palatal Advanced Flap: A Pedicle Flap For Primary Coverage of Immediately Placed ImplantsMárcia ChatelieNoch keine Bewertungen
- Rekonstruksi SCC Dengan Flap Lateral ForeheadDokument7 SeitenRekonstruksi SCC Dengan Flap Lateral Foreheadmichaeljt_md6463Noch keine Bewertungen
- 2020 Scroll Ligament Nasal TipDokument10 Seiten2020 Scroll Ligament Nasal TipJuliann PedroNoch keine Bewertungen
- Surgical Endodontics Cases 2Dokument59 SeitenSurgical Endodontics Cases 2Maryam Mohamed Abdelkarim AbdelfattahNoch keine Bewertungen
- Evaluation of The Effectiveness of Collagen Membrane in The Management of Oro Antral FistulaCommunication A Clinical StudyDokument8 SeitenEvaluation of The Effectiveness of Collagen Membrane in The Management of Oro Antral FistulaCommunication A Clinical StudyAthenaeum Scientific PublishersNoch keine Bewertungen
- 10.1007@s10006 019 00771 4Dokument5 Seiten10.1007@s10006 019 00771 4Karol Y. Wilson LondoñoNoch keine Bewertungen
- Initial Experience With Application of Single Layer Modified Kugel Mesh For Inguinal Hernia Repair: Case Series of 72 Consecutive PatientsDokument6 SeitenInitial Experience With Application of Single Layer Modified Kugel Mesh For Inguinal Hernia Repair: Case Series of 72 Consecutive Patientsnur hasnahNoch keine Bewertungen
- Use of Retroauricular Temporal Flap For Large Post Oncosurgical Glabellar and Forehead DefectsDokument4 SeitenUse of Retroauricular Temporal Flap For Large Post Oncosurgical Glabellar and Forehead DefectsPalwasha Malik100% (1)
- Sample Operative Report For 2014Dokument30 SeitenSample Operative Report For 2014Hemant KumarNoch keine Bewertungen
- The Forehead Flap For Nasal Degloving Injuries Reconstruction - A Case Report in Sanglah General Hospital DenpasarDokument15 SeitenThe Forehead Flap For Nasal Degloving Injuries Reconstruction - A Case Report in Sanglah General Hospital DenpasarGusti Ngurah PurnomoNoch keine Bewertungen
- Buccal FatDokument10 SeitenBuccal FatEmrys1987Noch keine Bewertungen
- Two Bilateral Zygomatic Implants Placed and Immediately Loaded A Retrospective Chart Review With Up-To-54-Month Follow-UpDokument5 SeitenTwo Bilateral Zygomatic Implants Placed and Immediately Loaded A Retrospective Chart Review With Up-To-54-Month Follow-UpBagis Emre Gul100% (1)
- Method of Reconstructive Operation For Patients With Nasal Deformation After Primary CheiloplastyDokument4 SeitenMethod of Reconstructive Operation For Patients With Nasal Deformation After Primary CheiloplastyCentral Asian StudiesNoch keine Bewertungen
- A Hollow Delayed Surgical ObturatorDokument55 SeitenA Hollow Delayed Surgical ObturatorvinnycoolbuddyNoch keine Bewertungen
- The Advantages of External DR PDFDokument13 SeitenThe Advantages of External DR PDFalitNoch keine Bewertungen
- Reconstrucción Defectos Nasales PDFDokument18 SeitenReconstrucción Defectos Nasales PDFSara OmNoch keine Bewertungen
- Journal Pre-Proof: British Journal of Oral & Maxillofacial SurgeryDokument16 SeitenJournal Pre-Proof: British Journal of Oral & Maxillofacial Surgeryabhishekjha0082Noch keine Bewertungen
- Oncu 2017Dokument6 SeitenOncu 2017Jesse Coelho SchardosimNoch keine Bewertungen
- JC 16Dokument36 SeitenJC 16BharathSimhaReddyDalliNoch keine Bewertungen
- Case Report On Maxillary Labial FrenectomyDokument9 SeitenCase Report On Maxillary Labial Frenectomyviolita chresnaNoch keine Bewertungen
- Socket An OftalmicDokument15 SeitenSocket An OftalmicMonika Putong PaatNoch keine Bewertungen
- 10 1093@asj@sjaa018Dokument60 Seiten10 1093@asj@sjaa018Luiggi FayadNoch keine Bewertungen
- Cheek FlapDokument4 SeitenCheek FlapDae AhmadNoch keine Bewertungen
- Infrahyoid Flap, A Convenient Alternative For Reconstruction of Tongue and Floor of Mouth Defects: Case SeriesDokument4 SeitenInfrahyoid Flap, A Convenient Alternative For Reconstruction of Tongue and Floor of Mouth Defects: Case SeriesPedro TurraNoch keine Bewertungen
- A Modified Bilobed Flap Design For Nasal Tip DefecDokument5 SeitenA Modified Bilobed Flap Design For Nasal Tip DefecCPR tyoNoch keine Bewertungen
- Ir 2867Dokument8 SeitenIr 2867shamsshanti999Noch keine Bewertungen
- Top of Page Patients and Methods Results Discussion Conclusion BibliographyDokument16 SeitenTop of Page Patients and Methods Results Discussion Conclusion BibliographyentsrmcNoch keine Bewertungen
- Restoration of Soft Triangle of The Nose Using Auricular Composite Graft and Fibrin GlueDokument6 SeitenRestoration of Soft Triangle of The Nose Using Auricular Composite Graft and Fibrin GluePatricia CieloNoch keine Bewertungen
- Alogénico Vs AutoóogoDokument4 SeitenAlogénico Vs AutoóogoMaximiliano Jara ContrerasNoch keine Bewertungen
- Hard Palate Dermis Fat Composite Graft For Reconstruction of Contracted Anophthalmic SocketDokument7 SeitenHard Palate Dermis Fat Composite Graft For Reconstruction of Contracted Anophthalmic SocketSaraelsy MonterrosoNoch keine Bewertungen
- Asianrhinoplasty: Dean M. Toriumi,, Colin D. PeroDokument18 SeitenAsianrhinoplasty: Dean M. Toriumi,, Colin D. PerodrbantmNoch keine Bewertungen
- 3.a Comparative Study of EndoscopicDokument7 Seiten3.a Comparative Study of EndoscopicDR K C MALLIKNoch keine Bewertungen
- Aps 39 118Dokument8 SeitenAps 39 118isabelNoch keine Bewertungen
- Graftless Solutions for the Edentulous PatientVon EverandGraftless Solutions for the Edentulous PatientSaj JivrajNoch keine Bewertungen
- Analisis StatistikDokument3 SeitenAnalisis StatistikasepNoch keine Bewertungen
- Squamous CELL CARCINOMA Fix DNYDokument60 SeitenSquamous CELL CARCINOMA Fix DNYasepNoch keine Bewertungen
- Squamous CELL CARCINOMA Fix DNYDokument60 SeitenSquamous CELL CARCINOMA Fix DNYasepNoch keine Bewertungen
- InfeksiDokument22 SeitenInfeksiasepNoch keine Bewertungen
- Surgical Approaches For Condylar Fractures Related To FacialDokument34 SeitenSurgical Approaches For Condylar Fractures Related To FacialasepNoch keine Bewertungen
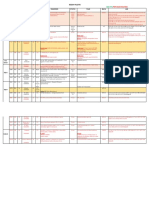
- Hari Identitas Diagnosis Tindakan DPJP Ket: Rencana Operasi Bedah Plastik 4-11 JanuariDokument1 SeiteHari Identitas Diagnosis Tindakan DPJP Ket: Rencana Operasi Bedah Plastik 4-11 JanuariasepNoch keine Bewertungen
- Bedah Plastik Selasa, 8 Januari 2019: Ruang Bed PJ DPJP Nama U MRS Diagnosis Status Plan Biaya LABDokument2 SeitenBedah Plastik Selasa, 8 Januari 2019: Ruang Bed PJ DPJP Nama U MRS Diagnosis Status Plan Biaya LABasepNoch keine Bewertungen
- Recent Publications On Myofunctional TherapyDokument5 SeitenRecent Publications On Myofunctional TherapyasepNoch keine Bewertungen
- Absen Apel 19 SepDokument1 SeiteAbsen Apel 19 SepasepNoch keine Bewertungen
- Antrian BangsalDokument1 SeiteAntrian BangsalasepNoch keine Bewertungen
- Serialextraction 2Dokument6 SeitenSerialextraction 2Zullia TaftyantiNoch keine Bewertungen
- BionatorDokument1 SeiteBionatorasepNoch keine Bewertungen
- Burn Caused Brain InjuredDokument12 SeitenBurn Caused Brain InjuredasepNoch keine Bewertungen
- Diagnosis & Treament: ShockDokument52 SeitenDiagnosis & Treament: ShockasepNoch keine Bewertungen
- HOD Whitening RPT PDFDokument13 SeitenHOD Whitening RPT PDFasepNoch keine Bewertungen
- Modern DesignDokument50 SeitenModern DesignasepNoch keine Bewertungen
- Dios 2005Dokument5 SeitenDios 2005asepNoch keine Bewertungen
- Reseksi en BlocDokument10 SeitenReseksi en Blocasep100% (1)
- Modern OrthodonticsDokument2 SeitenModern OrthodonticsasepNoch keine Bewertungen
- Cerebellum, Thalamus, and HypothalamusDokument40 SeitenCerebellum, Thalamus, and Hypothalamusasep100% (1)
- Analisis Sampel GpowerDokument1 SeiteAnalisis Sampel GpowerasepNoch keine Bewertungen
- Technique To Manage The EnlargedDokument16 SeitenTechnique To Manage The EnlargedasepNoch keine Bewertungen
- Oral Microorganism / Bacteria / Flora: EnvinronmentDokument3 SeitenOral Microorganism / Bacteria / Flora: EnvinronmentasepNoch keine Bewertungen
- Anatomical LandmarkDokument12 SeitenAnatomical LandmarkasepNoch keine Bewertungen
- Processing ErrorsDokument19 SeitenProcessing ErrorsasepNoch keine Bewertungen
- Processing ErrorsDokument19 SeitenProcessing ErrorsasepNoch keine Bewertungen
- Kesehatan Lingkungan Pada Sarana Pelayanan Kesehatan: Surartono D Bagian IKGM - KGP FKG UnejDokument20 SeitenKesehatan Lingkungan Pada Sarana Pelayanan Kesehatan: Surartono D Bagian IKGM - KGP FKG UnejasepNoch keine Bewertungen
- Kesling RSDokument20 SeitenKesling RSasepNoch keine Bewertungen
- Apakah Bentuk Atom SEPERTI............. : V.Montgomery & R.Smith 1Dokument113 SeitenApakah Bentuk Atom SEPERTI............. : V.Montgomery & R.Smith 1asepNoch keine Bewertungen
- Scenario Fall RcaDokument3 SeitenScenario Fall RcaPatient Safety MyNoch keine Bewertungen
- Dekker Surgical Atlas of Pediatric OtolaryngologyDokument865 SeitenDekker Surgical Atlas of Pediatric OtolaryngologyDaniel Rajkumar100% (2)
- Facial Feminization Surgery FFS Surgeon ListingsDokument46 SeitenFacial Feminization Surgery FFS Surgeon ListingsTrinity Rose Transsexual100% (2)
- Stamm Gastrostomy (Complete)Dokument6 SeitenStamm Gastrostomy (Complete)robelNoch keine Bewertungen
- UMDNS CODES Concept DefinitionsDokument2.942 SeitenUMDNS CODES Concept DefinitionsVictor Saldaña60% (5)
- Principles of Sterile Field and Definitions or Romm PresentationDokument29 SeitenPrinciples of Sterile Field and Definitions or Romm PresentationAprille Claire MoralesNoch keine Bewertungen
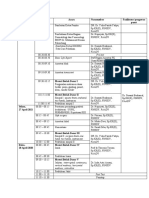
- Hari Waktu Acara Narasumber Fasilitator/ Pengawas Pusat Senin, 26 April 2021Dokument2 SeitenHari Waktu Acara Narasumber Fasilitator/ Pengawas Pusat Senin, 26 April 2021Larvahmir SpDVNoch keine Bewertungen
- Total Thyroidectomy - EdittedDokument55 SeitenTotal Thyroidectomy - EdittedPrisicilla Doydora Pat67% (3)
- Management of The Injured Hand - Basic PrinciplesDokument6 SeitenManagement of The Injured Hand - Basic PrinciplesIndah GitaswariNoch keine Bewertungen
- Client Information Form-Québec: FormtextDokument5 SeitenClient Information Form-Québec: FormtextJhullian Frederick Val VergaraNoch keine Bewertungen
- Flexible Intramedullary Nailing in Children The Nancy University ManualDokument319 SeitenFlexible Intramedullary Nailing in Children The Nancy University ManualMatej Miloš100% (1)
- Form 6 Revised 2022Dokument2 SeitenForm 6 Revised 2022Angelo AlcantaraNoch keine Bewertungen
- The American College of Surgeons, Minimum Standards For Hospitals, and The Provision of High-Quality Laboratory ServicesDokument14 SeitenThe American College of Surgeons, Minimum Standards For Hospitals, and The Provision of High-Quality Laboratory ServicesPamela Neyra VeraNoch keine Bewertungen
- Surgeine Disposable Gown Drape CatalogueDokument8 SeitenSurgeine Disposable Gown Drape CataloguebhawneshNoch keine Bewertungen
- ANSI/TIA 1179-A: Telecommunications InfrastructureDokument6 SeitenANSI/TIA 1179-A: Telecommunications InfrastructureFabio AssoniNoch keine Bewertungen
- BTK Implant Guide SurgeryDokument48 SeitenBTK Implant Guide SurgeryMaria VolvinaNoch keine Bewertungen
- Caldwell-Luc ProcedureDokument2 SeitenCaldwell-Luc ProcedureMaria NorilynNoch keine Bewertungen
- Letter of Intent Rmvega DvsDokument2 SeitenLetter of Intent Rmvega DvsZele VegaNoch keine Bewertungen
- @MedicalBooksStore 2015 Office Based PDFDokument237 Seiten@MedicalBooksStore 2015 Office Based PDFGalih WicaksonoNoch keine Bewertungen
- Essential Anesthesia From Science To Practice,.46Dokument1 SeiteEssential Anesthesia From Science To Practice,.46Jean PaulNoch keine Bewertungen
- Salko Zahirovic CV PDFDokument16 SeitenSalko Zahirovic CV PDFMehmed ImamovićNoch keine Bewertungen
- "Extreme" Cosmetic Surgery: A Retrospective Study of Morbidity in Patients Undergoing Combined ProceduresDokument5 Seiten"Extreme" Cosmetic Surgery: A Retrospective Study of Morbidity in Patients Undergoing Combined ProceduresDakirdaNoch keine Bewertungen
- Chemo ProphylaxisDokument13 SeitenChemo ProphylaxisSaket DaokarNoch keine Bewertungen
- VectraOwnersManual Feb07Dokument428 SeitenVectraOwnersManual Feb07salah subbahNoch keine Bewertungen
- CFS - File 1-3-14Dokument12 SeitenCFS - File 1-3-14Andri aryanataNoch keine Bewertungen
- PRPDokument9 SeitenPRPmutmainnah_kamilNoch keine Bewertungen
- Anaesthesia Resident's HandbookDokument445 SeitenAnaesthesia Resident's HandbookAnastasiafynn50% (2)
- Discharge Summary: Dept ofDokument2 SeitenDischarge Summary: Dept ofajjukujju1989Noch keine Bewertungen
- Interview GoodDokument4 SeitenInterview GoodchrisNoch keine Bewertungen
- EDRA Reading List v2Dokument3 SeitenEDRA Reading List v2MubeenRahmanNoch keine Bewertungen