Das könnte Ihnen auch gefallen
- Antineoplastic DrugsDokument16 SeitenAntineoplastic DrugstheintrovNoch keine Bewertungen
- Anti InfectivesDokument126 SeitenAnti Infectiveseunice lachicaNoch keine Bewertungen
- Study Questions Answered by Sir Charles MCDokument13 SeitenStudy Questions Answered by Sir Charles MCTakudzwa ChirumeNoch keine Bewertungen
- Pharmacology QuestionsDokument10 SeitenPharmacology QuestionsEthel Gretchen CasallaNoch keine Bewertungen
- NCM 106 Drugs Acting On ANS - Synchronous Session Ver 2Dokument7 SeitenNCM 106 Drugs Acting On ANS - Synchronous Session Ver 2Crecia Bullecer2Noch keine Bewertungen
- Infectious and Inflammatory Disorders of The Urinary SystemDokument16 SeitenInfectious and Inflammatory Disorders of The Urinary SystemBibi Renu100% (1)
- Mechanisms of Drug Toxicity: Proceedings of the Third International Pharmacological MeetingVon EverandMechanisms of Drug Toxicity: Proceedings of the Third International Pharmacological MeetingH. RaškováNoch keine Bewertungen
- Neurodegenerative DiseasesDokument32 SeitenNeurodegenerative DiseasesApurba Sarker Apu100% (1)
- Expanded Program On ImmunizationDokument15 SeitenExpanded Program On ImmunizationReygie MarsadaNoch keine Bewertungen
- Genitourinary Problem: Nephrotic Syndrome Wilm's Tumor ManagementDokument19 SeitenGenitourinary Problem: Nephrotic Syndrome Wilm's Tumor ManagementJayson CruzNoch keine Bewertungen
- Shock and SIRSDokument85 SeitenShock and SIRSBryan Mae H. DegorioNoch keine Bewertungen
- Pharm - Chapter - 13 - Central Nervous System StimulantsDokument42 SeitenPharm - Chapter - 13 - Central Nervous System StimulantsFeliciaDorghamNoch keine Bewertungen
- STDs Guide: Gonorrhea to SyphilisDokument5 SeitenSTDs Guide: Gonorrhea to Syphilisreghpineda28Noch keine Bewertungen
- Cervical CA Case StudyDokument32 SeitenCervical CA Case StudyCandy Mae Kabayao CuraNoch keine Bewertungen
- PHRM 246: MR Thabiso Tlaila Department of Pharmacology Discipline of Pharmaceutical Sciences University of Kwazulu-NatalDokument38 SeitenPHRM 246: MR Thabiso Tlaila Department of Pharmacology Discipline of Pharmaceutical Sciences University of Kwazulu-NatalSindile MchunuNoch keine Bewertungen
- Terminology of PsychiatryDokument6 SeitenTerminology of PsychiatryHassan.shehri100% (1)
- Medical Surgical: SNS (Anti-Cholinergic/adrenergic)Dokument12 SeitenMedical Surgical: SNS (Anti-Cholinergic/adrenergic)Pedro SorianoNoch keine Bewertungen
- Chapter 73: Drug Therapy of Rheumatoid Arthritis Test Bank: Multiple ChoiceDokument4 SeitenChapter 73: Drug Therapy of Rheumatoid Arthritis Test Bank: Multiple ChoiceNurse Utopia100% (1)
- Vasodilators: A B C D XDokument1 SeiteVasodilators: A B C D XPatricia Marie BuenafeNoch keine Bewertungen
- Neurologic Assessment Physiologic Changes With AgingDokument4 SeitenNeurologic Assessment Physiologic Changes With AgingDarl Dacdac100% (1)
- NUR100 Sherpath CH 44 PainDokument23 SeitenNUR100 Sherpath CH 44 Paincaloy2345caloyNoch keine Bewertungen
- Pharma Mod 11Dokument12 SeitenPharma Mod 11ANGELA SHANE AGUSTINNoch keine Bewertungen
- COMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideVon EverandCOMPREHENSIVE NURSING ACHIEVEMENT TEST (RN): Passbooks Study GuideNoch keine Bewertungen
- Gastrointestinal DrugsDokument2 SeitenGastrointestinal DrugsJannah Mikhaela Alibay VillarinNoch keine Bewertungen
- Pall CareDokument81 SeitenPall Careडा. सत्यदेव त्यागी आर्यNoch keine Bewertungen
- Endocrine System - DisorderDokument16 SeitenEndocrine System - Disordermajoi100% (1)
- Medication Errors & Risk ReductionDokument46 SeitenMedication Errors & Risk Reductionadni_wgNoch keine Bewertungen
- Cardiovascular Pharmacology PDFDokument20 SeitenCardiovascular Pharmacology PDFMelanie PrinceNoch keine Bewertungen
- Antiinflammatory Drugs: Toya AriawanDokument27 SeitenAntiinflammatory Drugs: Toya Ariawanlast100% (1)
- Inflammatory Disorders GuideDokument19 SeitenInflammatory Disorders GuideElla PaezNoch keine Bewertungen
- Anti InflammatoryDokument41 SeitenAnti InflammatoryKakai Ablanque LopozNoch keine Bewertungen
- IV FluidsDokument17 SeitenIV FluidsTiffany NicolèNoch keine Bewertungen
- Adaptation ModelDokument7 SeitenAdaptation ModelMichelle T. DimaanoNoch keine Bewertungen
- Mod Family Planning Final PDFDokument124 SeitenMod Family Planning Final PDFPatricia Anne EsmedillaNoch keine Bewertungen
- Safe SuctioningDokument31 SeitenSafe SuctioningKatrina Ponce100% (2)
- Revised Syllabus PharmacologyDokument15 SeitenRevised Syllabus PharmacologylouradelNoch keine Bewertungen
- AlcoholsDokument23 SeitenAlcoholsdhaineyNoch keine Bewertungen
- NCM 116 Module 3 and 4 PDFDokument183 SeitenNCM 116 Module 3 and 4 PDF7rvcnnxk88Noch keine Bewertungen
- Schizophrenia and Mental Health Nursing InterventionsDokument10 SeitenSchizophrenia and Mental Health Nursing InterventionsRosie CuasitoNoch keine Bewertungen
- Take Note: Task That Cannot Be Delegated (HOSPITAL)Dokument5 SeitenTake Note: Task That Cannot Be Delegated (HOSPITAL)Esha ReShaNoch keine Bewertungen
- Chapter 36 - Inflammatory & Structural Heart DisordersDokument6 SeitenChapter 36 - Inflammatory & Structural Heart Disordersjosie teehNoch keine Bewertungen
- Nurse Review: Medical-Surgical Nursing Endocrine System 2005Dokument215 SeitenNurse Review: Medical-Surgical Nursing Endocrine System 2005jonas2663Noch keine Bewertungen
- I. Introduction Peptic Ulcer Disease (PUD) IsDokument2 SeitenI. Introduction Peptic Ulcer Disease (PUD) Iszharmaine8Noch keine Bewertungen
- General Anesthetics AbeerDokument45 SeitenGeneral Anesthetics AbeerYousef JafarNoch keine Bewertungen
- Drugs Acting On The Immune SystemDokument33 SeitenDrugs Acting On The Immune SystemAnonymous iG0DCOf100% (1)
- Vitamin A Treatment and Measles PreventionDokument17 SeitenVitamin A Treatment and Measles PreventionJea VesagasNoch keine Bewertungen
- Clinical Haematology-Lecture SlidesDokument55 SeitenClinical Haematology-Lecture SlidesShiv Sookun100% (1)
- UntitledDokument20 SeitenUntitledstuffednurse100% (1)
- Levofloxacin 500mg Film-coated Tablets SmPC SummaryDokument10 SeitenLevofloxacin 500mg Film-coated Tablets SmPC SummaryOdunlamiNoch keine Bewertungen
- Cancer Risk Factors and Diagnostic TestsDokument33 SeitenCancer Risk Factors and Diagnostic TestsLaryn Ticuala50% (2)
- Alzheimer's Disease Causes, Effects, and TreatmentsDokument21 SeitenAlzheimer's Disease Causes, Effects, and TreatmentsJesshica Navarro AlejandrinoNoch keine Bewertungen
- Pharm Chapter 2 and 3 Study GuideDokument10 SeitenPharm Chapter 2 and 3 Study GuideamkNoch keine Bewertungen
- Anti Protozoal AgentsDokument19 SeitenAnti Protozoal AgentsNithish SNoch keine Bewertungen
- Pharma - SkinDokument8 SeitenPharma - Skinreference books100% (1)
- Asthma and COPD NCLEXDokument17 SeitenAsthma and COPD NCLEXPotchiee PfizerNoch keine Bewertungen
- The Nursing ProcessDokument9 SeitenThe Nursing Processiannello100% (2)
- Medical Surgical Nursing - LectureDokument77 SeitenMedical Surgical Nursing - LecturePink Majaila GludoNoch keine Bewertungen
- Nursing Care of Clients With Cardiovascular DisorderDokument16 SeitenNursing Care of Clients With Cardiovascular DisorderLuna MarieNoch keine Bewertungen
- Cardioactive DrugsDokument7 SeitenCardioactive DrugsleoNoch keine Bewertungen
- Complete Medical TermsDokument32 SeitenComplete Medical TermsSharifa Darayan100% (1)
- Pharmacology: Anti-InflammatoryDokument38 SeitenPharmacology: Anti-InflammatorySharifa DarayanNoch keine Bewertungen
- Autonomic Nervous System ExplainedDokument140 SeitenAutonomic Nervous System ExplainedSharifa Darayan100% (1)
- Pharmacology Important Things To RememberDokument5 SeitenPharmacology Important Things To RememberHydie100% (1)
- Biochem LabDokument14 SeitenBiochem LabSharifa DarayanNoch keine Bewertungen
- AntidepressantsDokument35 SeitenAntidepressantsKannahGraceLumabanNoch keine Bewertungen
- Pharmacology: EndocrineDokument210 SeitenPharmacology: EndocrineSharifa Darayan100% (1)
- Pharmacology: Cardiovascular SystemDokument314 SeitenPharmacology: Cardiovascular SystemSharifa DarayanNoch keine Bewertungen
- Pharmacology: AnalgesicsDokument84 SeitenPharmacology: AnalgesicsSharifa DarayanNoch keine Bewertungen
- ProteinsDokument14 SeitenProteinsSharifa DarayanNoch keine Bewertungen
- EnzymesDokument17 SeitenEnzymesSharifa DarayanNoch keine Bewertungen
- Diseases of The Urinary & Reproductive SystemDokument89 SeitenDiseases of The Urinary & Reproductive SystemSharifa DarayanNoch keine Bewertungen
- Group 4 Pathologies of The Respiratory System Report MicroDokument54 SeitenGroup 4 Pathologies of The Respiratory System Report MicroNapisa NajalNoch keine Bewertungen
- Essential Roles of Hospital PharmacistsDokument92 SeitenEssential Roles of Hospital PharmacistsabdrhmanNoch keine Bewertungen
- ART Guidelines for All PLHIVDokument41 SeitenART Guidelines for All PLHIVAshik Jithu JohnNoch keine Bewertungen
- Bumetanide MIMSDokument2 SeitenBumetanide MIMSIndri WahyuniNoch keine Bewertungen
- A Comparative Evaluation of Furosemide Tablets Marketed in LibyaDokument7 SeitenA Comparative Evaluation of Furosemide Tablets Marketed in LibyaMediterr J Pharm Pharm SciNoch keine Bewertungen
- Test Bank For Introduction To Clinical Pharmacology 6th Edition Marilyn EdmundsDokument9 SeitenTest Bank For Introduction To Clinical Pharmacology 6th Edition Marilyn EdmundsMitchellJohnsonktspjNoch keine Bewertungen
- Standard Operating Procedure For The Recording, Management and Reporting of Adverse Events by InvestigatorsDokument19 SeitenStandard Operating Procedure For The Recording, Management and Reporting of Adverse Events by Investigatorsvikram kushwahaNoch keine Bewertungen
- TC in 200 Pages PDFDokument195 SeitenTC in 200 Pages PDFWaleed MostafaNoch keine Bewertungen
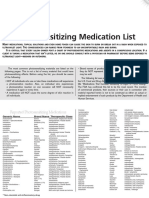
- Photosensitizing Medication ListDokument3 SeitenPhotosensitizing Medication ListDimas RfNoch keine Bewertungen
- Chemotherapy Sequencing Chart: Review Article Chemotherapy Administration SequenceDokument1 SeiteChemotherapy Sequencing Chart: Review Article Chemotherapy Administration SequencemubarakdxxNoch keine Bewertungen
- Daftar Pustaka FarmasiDokument3 SeitenDaftar Pustaka Farmasipermata putriNoch keine Bewertungen
- LDN Fact Sheet Provides Dosing and Mechanism DetailsDokument8 SeitenLDN Fact Sheet Provides Dosing and Mechanism DetailscristiNoch keine Bewertungen
- Terbinafine 250mgDokument14 SeitenTerbinafine 250mgddandan_2Noch keine Bewertungen
- State of Ohio Board of Pharmacy Reaches SettlementDokument3 SeitenState of Ohio Board of Pharmacy Reaches SettlementLydia TaylorNoch keine Bewertungen
- Cns Stimulant Activity of Aqueous Extract of Roots of Boerhavia Diffusa in MiceDokument4 SeitenCns Stimulant Activity of Aqueous Extract of Roots of Boerhavia Diffusa in MicerajenderizeNoch keine Bewertungen
- PSA MedsCheck GuidelinesDokument18 SeitenPSA MedsCheck GuidelinesRobbie WilliamsNoch keine Bewertungen
- The Accidental AddictsDokument6 SeitenThe Accidental AddictsnorthandsouthnzNoch keine Bewertungen
- Allopurinol Dosage, Classification, Indications, Adverse Reactions and Nursing ResponsibilitiesDokument1 SeiteAllopurinol Dosage, Classification, Indications, Adverse Reactions and Nursing ResponsibilitieskyawNoch keine Bewertungen
- Midterm Exam Review for Pharmacology Nursing StudentsDokument11 SeitenMidterm Exam Review for Pharmacology Nursing StudentsMark Jheran Alvarez100% (1)
- Stock List Material Medika Plaza PER 02 MARET 2021Dokument4 SeitenStock List Material Medika Plaza PER 02 MARET 2021medika plazaNoch keine Bewertungen
- Week5. Roles of PharmacistsDokument38 SeitenWeek5. Roles of PharmacistsKathleen GasparinNoch keine Bewertungen
- HCS Intro To Phar 1stDokument31 SeitenHCS Intro To Phar 1stGalataa MuktaarNoch keine Bewertungen
- PDF 0OIutGciNYy1qLCkgEMFDokument2 SeitenPDF 0OIutGciNYy1qLCkgEMFSusanta MohapatraNoch keine Bewertungen
- Group 2Dokument13 SeitenGroup 2arifpharmjuNoch keine Bewertungen
- Meet Top PFS Experts, Network With 100+ Pharma and Biotech Industry Leaders Next Week in BostonDokument3 SeitenMeet Top PFS Experts, Network With 100+ Pharma and Biotech Industry Leaders Next Week in BostonPR.comNoch keine Bewertungen
- Update of KetamineDokument12 SeitenUpdate of KetamineThoriqotil Haqqul MauludiyahNoch keine Bewertungen
- OBATDokument3 SeitenOBATCindy PrayogoNoch keine Bewertungen
- List Prof WiseDokument6 SeitenList Prof WiseHuma Hameed DogarNoch keine Bewertungen
- Form Stok Opname Gudang Farmasi Tanggal 26 Desember 2022 HPP Sisa Id Barang (Jangan Diubah) Nama (Jangan Diubah) ED (Jangan Diubah)Dokument30 SeitenForm Stok Opname Gudang Farmasi Tanggal 26 Desember 2022 HPP Sisa Id Barang (Jangan Diubah) Nama (Jangan Diubah) ED (Jangan Diubah)NovianaNoch keine Bewertungen
- Remember m2Dokument21 SeitenRemember m2Eman AlalawiNoch keine Bewertungen
- Drug Rules1986Dokument80 SeitenDrug Rules1986sadafNoch keine Bewertungen