Das könnte Ihnen auch gefallen
- Radiation Safety Procedures and Training for the Radiation Safety Officer: Guidance for Preparing a Radiation Safety ProgramVon EverandRadiation Safety Procedures and Training for the Radiation Safety Officer: Guidance for Preparing a Radiation Safety ProgramNoch keine Bewertungen
- Radiation Protection Bushong Study GuideDokument6 SeitenRadiation Protection Bushong Study GuideNanda Didana100% (1)
- Radiation Safety of X Ray Generators and Other Radiation Sources Used for Inspection Purposes and for Non-medical Human Imaging: Specific Safety GuideVon EverandRadiation Safety of X Ray Generators and Other Radiation Sources Used for Inspection Purposes and for Non-medical Human Imaging: Specific Safety GuideNoch keine Bewertungen
- Radiation Safety Series 3Dokument20 SeitenRadiation Safety Series 3johntobler100% (1)
- Radiographers - Radiation DosimetryDokument33 SeitenRadiographers - Radiation DosimetryAnonymous rYZyQQot55Noch keine Bewertungen
- Radiation Protection & Quality Assurance in CT 2018Dokument51 SeitenRadiation Protection & Quality Assurance in CT 2018abafzNoch keine Bewertungen
- Refresher & New User Training - 2005Dokument61 SeitenRefresher & New User Training - 2005Abdullah Ahd. AbdulrazigNoch keine Bewertungen
- Radiation Awareness Presentaion (Compatibility Mode)Dokument40 SeitenRadiation Awareness Presentaion (Compatibility Mode)AhmedAmer1100% (1)
- RSO (Medical) Exam SyllabusDokument4 SeitenRSO (Medical) Exam SyllabusSargunan SabNoch keine Bewertungen
- Radiation Protection 1Dokument51 SeitenRadiation Protection 1Mahnoor AqeelNoch keine Bewertungen
- Radiation DosimetryDokument18 SeitenRadiation DosimetrySmita SharmaNoch keine Bewertungen
- Radiation Safety ManualDokument21 SeitenRadiation Safety ManualNguyen Duc Dung100% (1)
- An Introduction To Radiation ProtectionDokument259 SeitenAn Introduction To Radiation ProtectionNabaaAlazawy89% (9)
- Lecture Notes Finals RT 208Dokument5 SeitenLecture Notes Finals RT 208Giralph NikkoNoch keine Bewertungen
- Radiation Monitoring Procedures in Hospital EnvironmentDokument5 SeitenRadiation Monitoring Procedures in Hospital Environmentnikkitha parker100% (1)
- Compton Academy 2023Dokument8 SeitenCompton Academy 2023Sargunan SabNoch keine Bewertungen
- Radiation Quantities & UnitsDokument31 SeitenRadiation Quantities & Unitsdeshpanderavi31100% (2)
- Radiation Safety PDFDokument67 SeitenRadiation Safety PDFHoàng Việt AnhNoch keine Bewertungen
- Piranha: Reference Manual - English - Version 5.5DDokument104 SeitenPiranha: Reference Manual - English - Version 5.5DFanof EcdNoch keine Bewertungen
- Radiation Biology LectureDokument39 SeitenRadiation Biology LectureBipin UpadhyayNoch keine Bewertungen
- Radiation Safety Short NotesDokument10 SeitenRadiation Safety Short Notesian3yeung-2Noch keine Bewertungen
- 2.37 Rso Training Standard Syllabi For Training Courses On Radiological SafetyDokument96 Seiten2.37 Rso Training Standard Syllabi For Training Courses On Radiological SafetyashwiniNoch keine Bewertungen
- Sample Problems BDokument8 SeitenSample Problems Bapi-308717184Noch keine Bewertungen
- Radiation Safety Series 2Dokument31 SeitenRadiation Safety Series 2johntoblerNoch keine Bewertungen
- Radiography QuizzesDokument11 SeitenRadiography QuizzesAwais JamilNoch keine Bewertungen
- Chapter 16 Radiation Protection and Safety PDFDokument236 SeitenChapter 16 Radiation Protection and Safety PDFAshutosh SinghNoch keine Bewertungen
- Radiation Safety Essay Ryan MonagoDokument5 SeitenRadiation Safety Essay Ryan Monagoapi-632682404Noch keine Bewertungen
- Question Bank On Radiation ProtectionDokument49 SeitenQuestion Bank On Radiation ProtectionAkhilesh Kumar100% (1)
- 06B Duties and Responsibilities of RSO RSRC 2018 EEIDokument27 Seiten06B Duties and Responsibilities of RSO RSRC 2018 EEIMichael Murillo BaraquioNoch keine Bewertungen
- 4 Background RadiationDokument1 Seite4 Background Radiationsomu1100% (1)
- Radiography Image Production and EvaluationDokument57 SeitenRadiography Image Production and EvaluationDally Rodriguez GammadNoch keine Bewertungen
- 4 PDFDokument90 Seiten4 PDFGopakumarNoch keine Bewertungen
- Shielding Calculations For Radiotherapy Calculation ExamplesDokument6 SeitenShielding Calculations For Radiotherapy Calculation ExamplesJuan DiazNoch keine Bewertungen
- Radiation ProtectionDokument50 SeitenRadiation ProtectionDragan GigiNoch keine Bewertungen
- RSD 4Dokument12 SeitenRSD 4GopakumarNoch keine Bewertungen
- RSO Book - Technology ExpertsDokument141 SeitenRSO Book - Technology ExpertsNaresh KumarNoch keine Bewertungen
- Radthera Exam Final 2022Dokument6 SeitenRadthera Exam Final 2022Marriel AmodiaNoch keine Bewertungen
- Radiation Safety PaperDokument4 SeitenRadiation Safety Paperapi-632827798Noch keine Bewertungen
- Lesson 2 QuizDokument1 SeiteLesson 2 Quizjohntobler0% (1)
- Discovery of RadiationDokument13 SeitenDiscovery of RadiationAdel SukerNoch keine Bewertungen
- Rad SafetyDokument5 SeitenRad Safetyapi-336647605Noch keine Bewertungen
- Rso QaDokument5 SeitenRso Qasrahman5229Noch keine Bewertungen
- RadiationDokument89 SeitenRadiationsugiarto80% (5)
- 02 Dose and Shielding Calculations RSRC 2018 EEIDokument48 Seiten02 Dose and Shielding Calculations RSRC 2018 EEIMichael Murillo Baraquio100% (1)
- Week 9 C Chapter 40 Radiation Protection, Chapter 31 QC 84Dokument84 SeitenWeek 9 C Chapter 40 Radiation Protection, Chapter 31 QC 84chicken66Noch keine Bewertungen
- Radiation Dose and Protection in DentistryDokument11 SeitenRadiation Dose and Protection in DentistryPhuong ThaoNoch keine Bewertungen
- Radiographic Artifacts 2Dokument56 SeitenRadiographic Artifacts 2Mac MacapilNoch keine Bewertungen
- Radiation Protection Bushong Study GuideDokument6 SeitenRadiation Protection Bushong Study GuideAsha6842100% (1)
- Radiation Protection Sample Q and ADokument20 SeitenRadiation Protection Sample Q and ARAD ROENTGENNoch keine Bewertungen
- Radiation Biology QuestionsDokument2 SeitenRadiation Biology QuestionsRoxy Marie ChanNoch keine Bewertungen
- Icrp 103Dokument328 SeitenIcrp 103Shiyama Swaminathan100% (1)
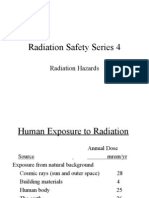
- Radiation Saftey Series 4Dokument26 SeitenRadiation Saftey Series 4johntoblerNoch keine Bewertungen
- Xray Training Anx - PPSXDokument54 SeitenXray Training Anx - PPSXkhurshedlakhoNoch keine Bewertungen
- Personnel Monitoring DevicesDokument63 SeitenPersonnel Monitoring DevicesPramod Tike100% (1)
- Occupational Radiation Safety: Directed Readings in The ClassroomDokument54 SeitenOccupational Radiation Safety: Directed Readings in The ClassroomErick Calcaligong100% (2)
- RADIOBIOLOGY Speaker Sharib Ahmed On 19-11-2013Dokument32 SeitenRADIOBIOLOGY Speaker Sharib Ahmed On 19-11-2013Waqar Ahmed0% (1)
- Radiography Practice Test-10Dokument4 SeitenRadiography Practice Test-10Chris Jordan100% (1)
- Bushong Rad ProtectionDokument7 SeitenBushong Rad ProtectionbbkanilNoch keine Bewertungen
- General Radio Graphic Image QualityDokument9 SeitenGeneral Radio Graphic Image QualityRouben ParmanumNoch keine Bewertungen
- Radiographers - Radiation DosimetryDokument33 SeitenRadiographers - Radiation Dosimetryd3trrNoch keine Bewertungen
- 7 ODE 2nd Order v2Dokument3 Seiten7 ODE 2nd Order v2Agung GuskaNoch keine Bewertungen
- PPT1 - Chemistry 1Dokument27 SeitenPPT1 - Chemistry 1mmsoledadNoch keine Bewertungen
- Understanding The Self Midterm Exam - PasigDokument1 SeiteUnderstanding The Self Midterm Exam - PasigEarl Tyrone P. Blanco100% (1)
- Zhong-Lin Lu, Barbara Dosher-Visual Psychophysics - From Laboratory To Theory-The MIT Press (2013)Dokument465 SeitenZhong-Lin Lu, Barbara Dosher-Visual Psychophysics - From Laboratory To Theory-The MIT Press (2013)IrinaNoch keine Bewertungen
- DIGSI4 Process Data AnalysisDokument27 SeitenDIGSI4 Process Data Analysismohammed youisfNoch keine Bewertungen
- MQL For Traders PDFDokument129 SeitenMQL For Traders PDFgorkemkebirNoch keine Bewertungen
- Deloitte Sample PapersDokument8 SeitenDeloitte Sample PapersAjay kumar TNPNoch keine Bewertungen
- Mahin Rahaman RESUMEDokument1 SeiteMahin Rahaman RESUMEMahin RahamanNoch keine Bewertungen
- Parts of The Microscope Quiz PDFDokument2 SeitenParts of The Microscope Quiz PDFEnriele De GuzmanNoch keine Bewertungen
- Revolutionize Your Business With The Industrial Internet of Things (IIoT)Dokument16 SeitenRevolutionize Your Business With The Industrial Internet of Things (IIoT)Sarah Walker100% (1)
- Why Slabs Curl - Part1Dokument6 SeitenWhy Slabs Curl - Part1Tim LinNoch keine Bewertungen
- Idemitsu - Super Multi Oil SeriesDokument2 SeitenIdemitsu - Super Multi Oil SeriesarieprachmanNoch keine Bewertungen
- Chapter 2 - Consumer Behavior - Market SegmentationDokument26 SeitenChapter 2 - Consumer Behavior - Market SegmentationAhmed RaufNoch keine Bewertungen
- Brochure PDFDokument1 SeiteBrochure PDFAstro Gourav100% (1)
- Full HRM Notes by Ram Chad Ran SirDokument122 SeitenFull HRM Notes by Ram Chad Ran SirKrupa PatilNoch keine Bewertungen
- Mothership ConnectionDokument10 SeitenMothership ConnectionTruman Dhanish100% (1)
- Pierderea Auzului Cauzata de Afectarea Transmiterii Sunetelor (Surditatea de Transmisie) : SunteleDokument3 SeitenPierderea Auzului Cauzata de Afectarea Transmiterii Sunetelor (Surditatea de Transmisie) : SunteleBianca AndreeaNoch keine Bewertungen
- Value of LifeDokument53 SeitenValue of LifeTu Phu Hoang LeNoch keine Bewertungen
- Lab #3Dokument10 SeitenLab #3Najmul Puda PappadamNoch keine Bewertungen
- How To OSCPDokument34 SeitenHow To OSCPbudi.hw748100% (3)
- PUP Manual EnglishDokument455 SeitenPUP Manual EnglishCharo Pajuelo ChaskaNoch keine Bewertungen
- Fieldcrest Division of Fieldcrest MillsDokument3 SeitenFieldcrest Division of Fieldcrest Millsmayur2510.20088662Noch keine Bewertungen
- Bhabha Atomic Research Centre BARC, MysuruDokument2 SeitenBhabha Atomic Research Centre BARC, Mysururajesh kumarNoch keine Bewertungen
- Unit N°1: Institucion Educativa Politécnico de Soledad English 10ThDokument3 SeitenUnit N°1: Institucion Educativa Politécnico de Soledad English 10ThMaria EscolarNoch keine Bewertungen
- Statement of PurposeDokument3 SeitenStatement of PurposeSamarth NegiNoch keine Bewertungen
- Theoretical Foundation in NursingDokument24 SeitenTheoretical Foundation in NursingJorie RocoNoch keine Bewertungen
- Lesson Plan in Science 3Dokument7 SeitenLesson Plan in Science 3renroseloraNoch keine Bewertungen
- Berna1Dokument4 SeitenBerna1Kenneth RomanoNoch keine Bewertungen
- 2016/2017 Master Timetable (Tentative) : Published: May 2016Dokument19 Seiten2016/2017 Master Timetable (Tentative) : Published: May 2016Ken StaynerNoch keine Bewertungen
- 3VA System Manual Communication en en-USDokument278 Seiten3VA System Manual Communication en en-UScraigjsandersonNoch keine Bewertungen