Das könnte Ihnen auch gefallen
- PolytraumaDokument64 SeitenPolytraumaOkkie Mharga SentanaNoch keine Bewertungen
- Thoracic Trauma - Navy - PSPD 2021Dokument45 SeitenThoracic Trauma - Navy - PSPD 2021Naavy LaksmonoNoch keine Bewertungen
- Initial Assessment and Management of Trauma PatientsDokument8 SeitenInitial Assessment and Management of Trauma PatientsAlvin De LunaNoch keine Bewertungen
- Polytrauma: DR A.R.Baka Department of Surgery Federal Medical Center, YolaDokument57 SeitenPolytrauma: DR A.R.Baka Department of Surgery Federal Medical Center, YolaAbuhafezbaka100% (1)
- Diagnosis and Treatment of Intraabdominal InjuriesDokument88 SeitenDiagnosis and Treatment of Intraabdominal Injuriessgod34Noch keine Bewertungen
- Initial Assessment and Management: Presented by Fayez Abillama, MDDokument53 SeitenInitial Assessment and Management: Presented by Fayez Abillama, MDDaniel GhosseinNoch keine Bewertungen
- 766 - HPS - Emergency TKVDokument82 Seiten766 - HPS - Emergency TKVAdistyDWNoch keine Bewertungen
- Trauma Assessment: Aims of The Initial Evaluation of Trauma PatientsDokument6 SeitenTrauma Assessment: Aims of The Initial Evaluation of Trauma Patientsece142Noch keine Bewertungen
- Initial Assessment and Management of Multiply Injured PatientsDokument30 SeitenInitial Assessment and Management of Multiply Injured PatientsSikaNoch keine Bewertungen
- Early Warning Score & Rapid Response TeamDokument26 SeitenEarly Warning Score & Rapid Response TeamAsim IdreesNoch keine Bewertungen
- Multiple Trauma ManagementDokument1 SeiteMultiple Trauma ManagementSetiawan Arif WibowoNoch keine Bewertungen
- Slide Jurnal BTKVDokument14 SeitenSlide Jurnal BTKVVistaririnNoch keine Bewertungen
- Torso TraumaDokument58 SeitenTorso TraumaAbidisHereNoch keine Bewertungen
- Thoracic Trauma ManagementDokument122 SeitenThoracic Trauma ManagementMarina Maleș100% (1)
- ATLS Student Manual Ch 1-13Dokument29 SeitenATLS Student Manual Ch 1-13Fahmi AnshoriNoch keine Bewertungen
- Everything You Need to Know About Flail Chest InjuriesDokument21 SeitenEverything You Need to Know About Flail Chest InjuriesOkagbue IzuchukwuNoch keine Bewertungen
- Abdominal Trauma: Supervised By: Dr. Hussein Al-HeisDokument63 SeitenAbdominal Trauma: Supervised By: Dr. Hussein Al-HeisRashed ShatnawiNoch keine Bewertungen
- Trauma OverviewDokument48 SeitenTrauma OverviewFrancescoBarbero100% (1)
- ATLS Initial Assessment and ManagementDokument21 SeitenATLS Initial Assessment and Managementazisfitri100% (2)
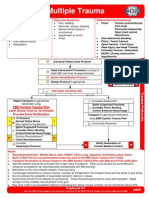
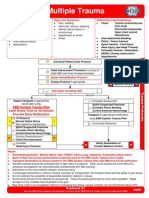
- Multiple Trauma: EMS System Trauma Plan Limit Scene Time To 10 Minutes Provide Early NotificationDokument1 SeiteMultiple Trauma: EMS System Trauma Plan Limit Scene Time To 10 Minutes Provide Early NotificationKelly JacksonNoch keine Bewertungen
- Understanding Mechanical Ventilation Modes & WeaningDokument52 SeitenUnderstanding Mechanical Ventilation Modes & WeaningDeepa BhattacharjeeNoch keine Bewertungen
- Trauma Protocol Manual Final 2012 WordDokument250 SeitenTrauma Protocol Manual Final 2012 WordelaNoch keine Bewertungen
- Anal Fissure Causes, Symptoms, and TreatmentDokument7 SeitenAnal Fissure Causes, Symptoms, and Treatmentashar khanNoch keine Bewertungen
- ABCs of Thoracic TraumaDokument5 SeitenABCs of Thoracic TraumaAlice S ChangNoch keine Bewertungen
- Ccam N Bps Management PDFDokument9 SeitenCcam N Bps Management PDFEthan AmalNoch keine Bewertungen
- S1M3 Update Fluid Resuscitation Management in Emergency CasesDokument70 SeitenS1M3 Update Fluid Resuscitation Management in Emergency Casesgriya medicaNoch keine Bewertungen
- ATLS DRDokument45 SeitenATLS DRNeNeei HenNieNoch keine Bewertungen
- Abdomen Injury-Dr - SayedDokument48 SeitenAbdomen Injury-Dr - SayedAnonymous xmw6mrNoch keine Bewertungen
- TRAUMA ORGAN ABDOMEN: ASSESSMENT AND MANAGEMENT OF BLUNT AND PENETRATING ABDOMINAL TRAUMADokument47 SeitenTRAUMA ORGAN ABDOMEN: ASSESSMENT AND MANAGEMENT OF BLUNT AND PENETRATING ABDOMINAL TRAUMAreginaNoch keine Bewertungen
- Student Refresher CourseDokument87 SeitenStudent Refresher CourseRaisa S. MariscalNoch keine Bewertungen
- Parade Bedah PlastikDokument28 SeitenParade Bedah PlastikMinarni HoNoch keine Bewertungen
- Pancreatitis: Dr. Ahmad Aqel RN, PHD The University of Jordan 2015Dokument27 SeitenPancreatitis: Dr. Ahmad Aqel RN, PHD The University of Jordan 2015Anonymous 5HzElnmNoch keine Bewertungen
- ICU Prophylaxis ChecklistDokument41 SeitenICU Prophylaxis ChecklistBharti NaraNoch keine Bewertungen
- Atls Approach To Pediatric TraumaDokument8 SeitenAtls Approach To Pediatric TraumaMakoto KyogokuNoch keine Bewertungen
- Terapi PaliatifDokument46 SeitenTerapi PaliatifViviViviNoch keine Bewertungen
- B.1 Applied Anatomy of Thorax - Asisten 2015 2Dokument126 SeitenB.1 Applied Anatomy of Thorax - Asisten 2015 2Stefany FanyNoch keine Bewertungen
- TriageDokument40 SeitenTriagemody94546Noch keine Bewertungen
- Initial Assessment and Management of the Multiply Injured PatientDokument48 SeitenInitial Assessment and Management of the Multiply Injured PatientDeep Katyan DeepNoch keine Bewertungen
- Cardiac Tamponade: Signs, Symptoms and DiagnosisDokument20 SeitenCardiac Tamponade: Signs, Symptoms and Diagnosismuhammad iqbal mahfuzhNoch keine Bewertungen
- Primary Trauma CareDokument48 SeitenPrimary Trauma CareKABERA RENENoch keine Bewertungen
- Woundcare Abdominal Wound Manado FinalDokument38 SeitenWoundcare Abdominal Wound Manado FinalDima F. PrawestiNoch keine Bewertungen
- Chest Tube and Water-Seal DrainageDokument25 SeitenChest Tube and Water-Seal DrainageGhadaNoch keine Bewertungen
- Chest Tube Drainage of The Pleural SpaceDokument10 SeitenChest Tube Drainage of The Pleural SpaceFernandaNoch keine Bewertungen
- Tracheostomy Procedure and CareDokument3 SeitenTracheostomy Procedure and CareSarah Elizabeth WalkerNoch keine Bewertungen
- Chest Trauma and Diseases: Mexigin Gayatri Akash JohannaDokument80 SeitenChest Trauma and Diseases: Mexigin Gayatri Akash JohannadidiNoch keine Bewertungen
- Canadian Triage and Acuity Scale for PediatricsDokument30 SeitenCanadian Triage and Acuity Scale for PediatricsPrince Jhessie L. AbellaNoch keine Bewertungen
- Diagnostic Thoracoscopy (VATS) in Lung CancerDokument18 SeitenDiagnostic Thoracoscopy (VATS) in Lung CancerlmdarlongNoch keine Bewertungen
- Liver Trauma: DR Tarik El Batrawy Specialist General SurgeryDokument50 SeitenLiver Trauma: DR Tarik El Batrawy Specialist General Surgerykata61Noch keine Bewertungen
- Tracheostomy Procedure GuideDokument10 SeitenTracheostomy Procedure GuideAinur AbdrakhmanovaNoch keine Bewertungen
- Basic Concept of BLS: Muhammad SaleemDokument27 SeitenBasic Concept of BLS: Muhammad Saleemms khanNoch keine Bewertungen
- Trauma Thorax Atls 9 Edition: Amatillah RaifahDokument20 SeitenTrauma Thorax Atls 9 Edition: Amatillah RaifahAnnifa RaifaNoch keine Bewertungen
- Abdominal and Pelvic Injury: Associate Professor Visokai V., PH.DDokument65 SeitenAbdominal and Pelvic Injury: Associate Professor Visokai V., PH.DRoman Mamun100% (1)
- PolitraumaDokument9 SeitenPolitraumaemo230485Noch keine Bewertungen
- ABC AbdomenDokument57 SeitenABC AbdomenSyahmi KhalidNoch keine Bewertungen
- Damage Control ResuscitationDokument24 SeitenDamage Control ResuscitationPaulShaneHerreraZorrillaNoch keine Bewertungen
- TracheostomyDokument56 SeitenTracheostomyRoshana MallawaarachchiNoch keine Bewertungen
- Emergency Airway Management TechniquesDokument31 SeitenEmergency Airway Management TechniquesNurul AfifahNoch keine Bewertungen
- ICU Scoring Systems A Complete Guide - 2020 EditionVon EverandICU Scoring Systems A Complete Guide - 2020 EditionNoch keine Bewertungen
- A Case-Based Approach to Interventional Pulmonology: A Focus on Asian PerspectivesVon EverandA Case-Based Approach to Interventional Pulmonology: A Focus on Asian PerspectivesJamalul Azizi Abdul RahamanNoch keine Bewertungen
- Addis Ababa University Faculty of Medicine Difficult Airway ManagementDokument54 SeitenAddis Ababa University Faculty of Medicine Difficult Airway ManagementagatakassaNoch keine Bewertungen
- A Descriptive Study To Assess The Knowledge and Practice Regarding Ventilator Associated Pneumonia VAP Critical Care Bundle Among Students of Selected Nursing Colleges of Distt. Mohali, PunjabDokument5 SeitenA Descriptive Study To Assess The Knowledge and Practice Regarding Ventilator Associated Pneumonia VAP Critical Care Bundle Among Students of Selected Nursing Colleges of Distt. Mohali, PunjabEditor IJTSRDNoch keine Bewertungen
- Crisis Management ManualDokument86 SeitenCrisis Management Manualemergs100% (2)
- Advance Airway MXDokument17 SeitenAdvance Airway MXMardhiyah MusaNoch keine Bewertungen
- Lasers in Maxillofacial Surgery and Dentistry 0865775664 PDFDokument168 SeitenLasers in Maxillofacial Surgery and Dentistry 0865775664 PDFIrina OneaNoch keine Bewertungen
- HFO Training ManualDokument396 SeitenHFO Training ManualMehek KhannaNoch keine Bewertungen
- Itls 9th Edition Prep Packet Advanced Provider VersionDokument19 SeitenItls 9th Edition Prep Packet Advanced Provider VersionUmidagha BaghirzadaNoch keine Bewertungen
- Nejm 2204556Dokument11 SeitenNejm 2204556tommy taylor084Noch keine Bewertungen
- Benumof and Hagberg's Airway Management (2012, Saunders) PDFDokument1.314 SeitenBenumof and Hagberg's Airway Management (2012, Saunders) PDFmodreanu andreiNoch keine Bewertungen
- Soal Post TestDokument70 SeitenSoal Post Testananda96% (25)
- Final Anaesthesia QuestionsDokument23 SeitenFinal Anaesthesia QuestionsRancesh FamoNoch keine Bewertungen
- Paramedic NREMTDokument88 SeitenParamedic NREMTJadie Barringer III100% (2)
- Laryngospasm CC 2Dokument18 SeitenLaryngospasm CC 2lilliansilvaNoch keine Bewertungen
- Flexible CO2 Laser Treatment For Subglottic Stenosis, 2017Dokument2 SeitenFlexible CO2 Laser Treatment For Subglottic Stenosis, 2017Araceli BarreraNoch keine Bewertungen
- Newborn Resuscitation..Dokument125 SeitenNewborn Resuscitation..Rahul DhakerNoch keine Bewertungen
- Ramos Vs CA - 124354 - April 11, 2002 - J. Kapunan - First DIvisionDokument24 SeitenRamos Vs CA - 124354 - April 11, 2002 - J. Kapunan - First DIvisionjonbelzaNoch keine Bewertungen
- Trauma Team 2007Dokument5 SeitenTrauma Team 2007Christopher TorresNoch keine Bewertungen
- Demonstration On NALSDokument20 SeitenDemonstration On NALSMary MenuNoch keine Bewertungen
- Procedure for Extubation and DecannulationDokument5 SeitenProcedure for Extubation and Decannulationydtrgn100% (1)
- ITLS 9e Advanced Pre-Test - Version 9.2 - Answer KeysDokument11 SeitenITLS 9e Advanced Pre-Test - Version 9.2 - Answer KeysNeil Thomas88% (8)
- Caring For Mechanical Ventilated PatientDokument10 SeitenCaring For Mechanical Ventilated Patientems100% (1)
- Thesis TopicsDokument7 SeitenThesis TopicsShoyeb Khan100% (1)
- Product CatalogDokument105 SeitenProduct CatalogsyitaNoch keine Bewertungen
- Teaching Learning Guide (Assist and NGT Insertion)Dokument12 SeitenTeaching Learning Guide (Assist and NGT Insertion)BeanncaAngeles100% (1)
- Interventional BronchosDokument323 SeitenInterventional BronchosSmaranda Demian100% (2)
- Pediatric Advanced Life Support (PALS) - 19-8-19Dokument36 SeitenPediatric Advanced Life Support (PALS) - 19-8-19RimaWulandari50% (2)
- NRP 1Dokument12 SeitenNRP 1syasyaNoch keine Bewertungen
- Management of Life Threatening Asthma. Severe Asthma Series. CHEST 2022Dokument10 SeitenManagement of Life Threatening Asthma. Severe Asthma Series. CHEST 2022carla jazmin cortes rodriguezNoch keine Bewertungen
- Choanal AtresiaDokument7 SeitenChoanal AtresiaAmmar EidNoch keine Bewertungen
- PublicationDokument532 SeitenPublicationSoniaLluenPisfil100% (1)