Das könnte Ihnen auch gefallen
- Effective Communication Chapter11Dokument9 SeitenEffective Communication Chapter11kamaljeet70Noch keine Bewertungen
- Ba GastrectomyDokument10 SeitenBa GastrectomyHope3750% (2)
- Degeneration & Regeneration of Nerve FibreDokument29 SeitenDegeneration & Regeneration of Nerve FibreSana FatimaNoch keine Bewertungen
- WatsuDokument5 SeitenWatsuTIME-TREVELER100% (1)
- Fracture Healing: Dow University of Health SciencesDokument15 SeitenFracture Healing: Dow University of Health SciencesZaheer KhanNoch keine Bewertungen
- Bone HealingDokument5 SeitenBone HealingFadliArifNoch keine Bewertungen
- 1.1 Biology of Bone HealingDokument32 Seiten1.1 Biology of Bone HealingCristian CumpănăNoch keine Bewertungen
- Lect 2 Membrane TransportDokument29 SeitenLect 2 Membrane Transportramadan100% (1)
- Tissue Renewal, Regeneration and RepairDokument50 SeitenTissue Renewal, Regeneration and RepairNurul AfiahNoch keine Bewertungen
- Palatine TonsilsDokument16 SeitenPalatine TonsilsK.charitha ChowdaryNoch keine Bewertungen
- Physiology of Respiration: Course Code: BBS01T1008 Course Name: Biology For EngineersDokument15 SeitenPhysiology of Respiration: Course Code: BBS01T1008 Course Name: Biology For EngineersDivya TripathyNoch keine Bewertungen
- Inflammation PPT - OdpDokument82 SeitenInflammation PPT - OdpBhanu PraseedhaNoch keine Bewertungen
- Fracture: Presented By: Ms. Durga Joshi M. SC NursingDokument63 SeitenFracture: Presented By: Ms. Durga Joshi M. SC NursingSanjaya PutraNoch keine Bewertungen
- Chapter 4 Tissues, Glands, and MembranesDokument11 SeitenChapter 4 Tissues, Glands, and MembranesMaria Angela Del Gallego100% (2)
- Cardiovascular System: More Than Just The HeartDokument34 SeitenCardiovascular System: More Than Just The HearteliseudesafateNoch keine Bewertungen
- ShockDokument64 SeitenShockAnusha VergheseNoch keine Bewertungen
- BMT ReportDokument26 SeitenBMT ReportCaroline AgbayNoch keine Bewertungen
- Otitis MediaDokument9 SeitenOtitis MediaMona Santi NainggolanNoch keine Bewertungen
- Physical Examination and Health Assessment: Genitourinary SystemDokument134 SeitenPhysical Examination and Health Assessment: Genitourinary Systemmesfin DemiseNoch keine Bewertungen
- An Organ That Receives and Relays Information About The Body's Senses To The BrainDokument59 SeitenAn Organ That Receives and Relays Information About The Body's Senses To The BrainIsarra AmsaluNoch keine Bewertungen
- Structure of Digestive SystemDokument8 SeitenStructure of Digestive System32 Mhd RayisNoch keine Bewertungen
- Therapy (LLL)Dokument432 SeitenTherapy (LLL)Biruk DesalegnNoch keine Bewertungen
- Syncope: - Selvarathi KDokument27 SeitenSyncope: - Selvarathi KSelvarathi KandhaswamyNoch keine Bewertungen
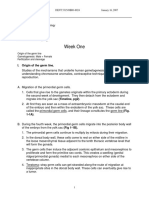
- Week One: I. Origin of The Germ LineDokument67 SeitenWeek One: I. Origin of The Germ LinerohitNoch keine Bewertungen
- Chapter 9 - Muscular System: Three Types of Muscle TissuesDokument73 SeitenChapter 9 - Muscular System: Three Types of Muscle TissuesRafie HusniNoch keine Bewertungen
- Calcium Homeostasis: Endocrine Regulation of (Ca)Dokument4 SeitenCalcium Homeostasis: Endocrine Regulation of (Ca)PRANAB KUMAR MUKHERJEENoch keine Bewertungen
- Approach To An Unconscious Patient-OyeyemiDokument41 SeitenApproach To An Unconscious Patient-OyeyemiOyeyemi AdeyanjuNoch keine Bewertungen
- Rectum & Anal CanalDokument14 SeitenRectum & Anal CanalLisa DentonNoch keine Bewertungen
- Tissues, Glands and MembranesDokument68 SeitenTissues, Glands and MembranesMerrylFrancisco100% (1)
- Development of The FaceDokument76 SeitenDevelopment of The Facedr parveen bathla100% (1)
- Burns Practice TeachingDokument58 SeitenBurns Practice TeachingSakthi Devi100% (1)
- Presented By: DR Sharmila G SDokument76 SeitenPresented By: DR Sharmila G SSharmila Shivakumar G SNoch keine Bewertungen
- Skin and Body MembranesDokument7 SeitenSkin and Body MembranesJoanna Carla Marmonejo Estorninos-Walker100% (2)
- CT KubDokument2 SeitenCT KubKumail KhandwalaNoch keine Bewertungen
- Woundhealingseminar 150216070848 Conversion Gate02Dokument103 SeitenWoundhealingseminar 150216070848 Conversion Gate02mohan100% (1)
- Clinical HYPERTENSION LecDokument44 SeitenClinical HYPERTENSION LecFarwaNoch keine Bewertungen
- InfluenzaDokument16 SeitenInfluenzaTrue AlphaNoch keine Bewertungen
- Human Anatomy,: First Edition Mckinley & O'LoughlinDokument40 SeitenHuman Anatomy,: First Edition Mckinley & O'LoughlinAgung PurmanaNoch keine Bewertungen
- Organ Transplant BenefitDokument7 SeitenOrgan Transplant BenefitenvadNoch keine Bewertungen
- Bleeding Per RectumeDokument35 SeitenBleeding Per RectumetharakaNoch keine Bewertungen
- Anatomy and Physiology Ii SMS 1224: Norhayati Ismail NOV 2011Dokument50 SeitenAnatomy and Physiology Ii SMS 1224: Norhayati Ismail NOV 2011Shirley LourdesNoch keine Bewertungen
- Embolism and InfarctionDokument34 SeitenEmbolism and InfarctionDiviya ArikrishnanNoch keine Bewertungen
- 16 Sense OrgansDokument79 Seiten16 Sense OrgansvanderphysNoch keine Bewertungen
- Digestive and Body MetabolismDokument25 SeitenDigestive and Body MetabolismGuenNoch keine Bewertungen
- Head Injury NoteDokument7 SeitenHead Injury NoteAi Mio100% (1)
- Class - Burns, Skin Graft & FlapsDokument44 SeitenClass - Burns, Skin Graft & FlapsJyoti Sambharwal100% (1)
- Embryology of HeartDokument16 SeitenEmbryology of HeartgetnusNoch keine Bewertungen
- Head To Toe ExaminationDokument6 SeitenHead To Toe ExaminationFadillah Raisyah MNoch keine Bewertungen
- Distribution of DrugsDokument36 SeitenDistribution of DrugsKashar SaeedNoch keine Bewertungen
- Bone Formation & GrowthDokument3 SeitenBone Formation & GrowtherinNoch keine Bewertungen
- By Danish LatifDokument43 SeitenBy Danish LatifShimmering MoonNoch keine Bewertungen
- Hearing and EquilibriumDokument30 SeitenHearing and EquilibriumabdirizakNoch keine Bewertungen
- Stage of Fracture HealingDokument5 SeitenStage of Fracture HealingDimas AgungNoch keine Bewertungen
- Assisting For Application of POPDokument7 SeitenAssisting For Application of POPINSERVICE EDUCATIONNoch keine Bewertungen
- Seminar On Cellulitis: Ms. J - Sheela Rajakumari MSC Nursing 1 Year MMM College of NursingDokument20 SeitenSeminar On Cellulitis: Ms. J - Sheela Rajakumari MSC Nursing 1 Year MMM College of NursingSheela Raja Kumari100% (1)
- Cardiovascular System: K. Hariharan Iv Eee - 'B'Dokument33 SeitenCardiovascular System: K. Hariharan Iv Eee - 'B'Hari Haran100% (1)
- Leg UlcersDokument22 SeitenLeg UlcersMarera DomnicNoch keine Bewertungen
- Bone Marrow and Stem Cell TranspplantDokument28 SeitenBone Marrow and Stem Cell TranspplantVILLEJO JHOVIALENNoch keine Bewertungen
- Lymph SystemDokument7 SeitenLymph SystemghaiathNoch keine Bewertungen
- Overview of GI Tract FunctionsDokument85 SeitenOverview of GI Tract FunctionsDerón Asbery HolmesNoch keine Bewertungen
- Bone HealingDokument43 SeitenBone Healingdana3rftsNoch keine Bewertungen
- Fracture Healing: Presenter: DR Mugi Ortho ResidentDokument32 SeitenFracture Healing: Presenter: DR Mugi Ortho ResidentPhoenix MerchantsNoch keine Bewertungen
- Fracture Healing: Presenter: DR Mugi Moderator: DR KalandeDokument32 SeitenFracture Healing: Presenter: DR Mugi Moderator: DR KalandePhoenix MerchantsNoch keine Bewertungen
- Edge Marking 2001Dokument22 SeitenEdge Marking 2001Pankaj VatsaNoch keine Bewertungen
- BOS Basic Arthroscopy Course ProgrammeDokument4 SeitenBOS Basic Arthroscopy Course ProgrammePankaj VatsaNoch keine Bewertungen
- Pathogenesis and Clinical Aspects of Rheumatoid Arthritis: Ivan Padjen, Cem Gabay, Daniel AletahaDokument83 SeitenPathogenesis and Clinical Aspects of Rheumatoid Arthritis: Ivan Padjen, Cem Gabay, Daniel AletahaPankaj VatsaNoch keine Bewertungen
- Arthroscopy Course 1219 FlierDokument1 SeiteArthroscopy Course 1219 FlierPankaj VatsaNoch keine Bewertungen
- Recent Advances in Wrist & Tendon Surgery: VenueDokument1 SeiteRecent Advances in Wrist & Tendon Surgery: VenuePankaj VatsaNoch keine Bewertungen
- Prevention of Surgical Site Infections in Orthopaedic Surgery: A Synthesis of Current RecommendationsDokument16 SeitenPrevention of Surgical Site Infections in Orthopaedic Surgery: A Synthesis of Current RecommendationsPankaj VatsaNoch keine Bewertungen
- ISHKS 2018 BrochureDokument11 SeitenISHKS 2018 BrochurePankaj VatsaNoch keine Bewertungen
- Ortho P-Iv ADokument1 SeiteOrtho P-Iv APankaj VatsaNoch keine Bewertungen
- 2 International Conference & Cadaveric Workshop On Pelviacetabular Fracture and Hip ArthrosDokument2 Seiten2 International Conference & Cadaveric Workshop On Pelviacetabular Fracture and Hip ArthrosPankaj VatsaNoch keine Bewertungen
- Orthopedics P - Iv June15 PDFDokument2 SeitenOrthopedics P - Iv June15 PDFPankaj VatsaNoch keine Bewertungen
- Brochure For AIOC Training JanuaryDokument4 SeitenBrochure For AIOC Training JanuaryPankaj VatsaNoch keine Bewertungen
- Cold Orthopaedic Cases PDFDokument1.039 SeitenCold Orthopaedic Cases PDFPankaj VatsaNoch keine Bewertungen
- Ortho P-Iii BDokument1 SeiteOrtho P-Iii BPankaj VatsaNoch keine Bewertungen
- Ortho P-Ii (B)Dokument1 SeiteOrtho P-Ii (B)Pankaj VatsaNoch keine Bewertungen
- Ortho P-I (B)Dokument1 SeiteOrtho P-I (B)Pankaj VatsaNoch keine Bewertungen
- Ortho P-Ii ADokument1 SeiteOrtho P-Ii APankaj VatsaNoch keine Bewertungen
- Ortho P-I (A)Dokument1 SeiteOrtho P-I (A)Pankaj VatsaNoch keine Bewertungen
- Ortho P-Ii BDokument1 SeiteOrtho P-Ii BPankaj VatsaNoch keine Bewertungen
- Epidemiology of Lumbar Disc HerniationDokument4 SeitenEpidemiology of Lumbar Disc HerniationPankaj VatsaNoch keine Bewertungen
- Ortho P-I BDokument1 SeiteOrtho P-I BPankaj VatsaNoch keine Bewertungen
- Final BasantDokument22 SeitenFinal BasantMuqaddas IsrarNoch keine Bewertungen
- IPA Digital Media Owners Survey Autumn 2010Dokument33 SeitenIPA Digital Media Owners Survey Autumn 2010PaidContentUKNoch keine Bewertungen
- MGMT 400-Strategic Business Management-Adnan ZahidDokument5 SeitenMGMT 400-Strategic Business Management-Adnan ZahidWaleed AhmadNoch keine Bewertungen
- Development Communication Theories MeansDokument13 SeitenDevelopment Communication Theories MeansKendra NodaloNoch keine Bewertungen
- Performance Task in Mathematics 10 First Quarter: GuidelinesDokument2 SeitenPerformance Task in Mathematics 10 First Quarter: Guidelinesbelle cutiee100% (3)
- Thermal (TE-411,412,413,414,511)Dokument25 SeitenThermal (TE-411,412,413,414,511)nved01Noch keine Bewertungen
- Sample ProposalDokument2 SeitenSample ProposaltoupieNoch keine Bewertungen
- Consumer Trend Canvas (CTC) Template 2022Dokument1 SeiteConsumer Trend Canvas (CTC) Template 2022Patricia DominguezNoch keine Bewertungen
- 10 Fonts For A Better WebsiteDokument3 Seiten10 Fonts For A Better WebsiteAlyzza Kara AcabalNoch keine Bewertungen
- Business Environment Analysis (Porter's 5 Forces Model)Dokument9 SeitenBusiness Environment Analysis (Porter's 5 Forces Model)FarihaNoch keine Bewertungen
- Durability Problems of 20 Century Reinforced Concrete Heritage Structures and Their RestorationsDokument120 SeitenDurability Problems of 20 Century Reinforced Concrete Heritage Structures and Their RestorationsManjunath ShepurNoch keine Bewertungen
- Rosemarie ManlapazDokument3 SeitenRosemarie ManlapazRonald ManlapazNoch keine Bewertungen
- RH Control - SeracloneDokument2 SeitenRH Control - Seraclonewendys rodriguez, de los santosNoch keine Bewertungen
- Eurokids Parent Manual (ECity) - PDF-EJ and ESDokument18 SeitenEurokids Parent Manual (ECity) - PDF-EJ and ESsabarin_72100% (2)
- 1654557191.969365 - Signed Contract Application 212143Dokument11 Seiten1654557191.969365 - Signed Contract Application 212143ella may sapilanNoch keine Bewertungen
- ESC Cardiomyopathy ClassificationDokument7 SeitenESC Cardiomyopathy Classificationvalerius83Noch keine Bewertungen
- 20 Great American Short Stories: Favorite Short Story Collections The Short Story LibraryDokument10 Seiten20 Great American Short Stories: Favorite Short Story Collections The Short Story Librarywileyh100% (1)
- Weekly Learning Plan: Department of EducationDokument2 SeitenWeekly Learning Plan: Department of EducationJim SulitNoch keine Bewertungen
- CB Insights Venture Report 2021Dokument273 SeitenCB Insights Venture Report 2021vulture212Noch keine Bewertungen
- Literature Review LichenDokument7 SeitenLiterature Review LichenNur Fazrina CGNoch keine Bewertungen
- Software Development Life CycleDokument70 SeitenSoftware Development Life CycleChaitanya MalikNoch keine Bewertungen
- Cyrano de BergeracDokument209 SeitenCyrano de BergeracKayleeNoch keine Bewertungen
- Timothy Ajani, "Syntax and People: How Amos Tutuola's English Was Shaped by His People"Dokument20 SeitenTimothy Ajani, "Syntax and People: How Amos Tutuola's English Was Shaped by His People"PACNoch keine Bewertungen
- Secant Method - Derivation: A. Bracketing MethodsDokument5 SeitenSecant Method - Derivation: A. Bracketing MethodsStephen Dela CruzNoch keine Bewertungen
- Risk AssessmentDokument38 SeitenRisk AssessmentYasar arafat SHNoch keine Bewertungen
- Taxation and LibertyDokument28 SeitenTaxation and LibertyRitu Raj RamanNoch keine Bewertungen
- Appraising The Secretaries of Sweet Water UniversityDokument4 SeitenAppraising The Secretaries of Sweet Water UniversityZain4uNoch keine Bewertungen