Das könnte Ihnen auch gefallen
- Arteri LineDokument13 SeitenArteri Linemuthia octavianaNoch keine Bewertungen
- Pulmonary Artery Catheterization and MonitoringDokument31 SeitenPulmonary Artery Catheterization and MonitoringVhince Norben PiscoNoch keine Bewertungen
- Arterial LineDokument2 SeitenArterial LineRaghav Goyal100% (1)
- Arterial LineDokument34 SeitenArterial Linepop lopNoch keine Bewertungen
- Hemodynamic Monitoring 1Dokument10 SeitenHemodynamic Monitoring 1Savita HanamsagarNoch keine Bewertungen
- Swan Ganz Catheterization GuideDokument24 SeitenSwan Ganz Catheterization GuideArchana Maharjan100% (1)
- Arterial Line Monitoring GuideDokument13 SeitenArterial Line Monitoring GuideberhanubedassaNoch keine Bewertungen
- Akses Vena Central: Anestesiologi Dan Reanimasi RSUD TasikmalayaDokument28 SeitenAkses Vena Central: Anestesiologi Dan Reanimasi RSUD TasikmalayaSaeful AmbariNoch keine Bewertungen
- Measuring Central Venous PressureDokument10 SeitenMeasuring Central Venous PressureRaghu RajanNoch keine Bewertungen
- Sister Nivedita Govt. Nursing College Igmc, ShimlaDokument10 SeitenSister Nivedita Govt. Nursing College Igmc, ShimlashivaniNoch keine Bewertungen
- Assisting With Arterial Puncture For Blood Gas Analysis EquipmentDokument7 SeitenAssisting With Arterial Puncture For Blood Gas Analysis EquipmentPoova RagavanNoch keine Bewertungen
- Umbilical Vein CatheterizationDokument3 SeitenUmbilical Vein CatheterizationrohitNoch keine Bewertungen
- Assessment - Blood PressureDokument3 SeitenAssessment - Blood PressuremArLoNNoch keine Bewertungen
- Patient Safety in HemodialysisDokument26 SeitenPatient Safety in HemodialysisMarivic Diano100% (2)
- Group3 - Sunico, Valenzuna, VelezDokument15 SeitenGroup3 - Sunico, Valenzuna, VelezMichelle SunicoNoch keine Bewertungen
- PERICARDIOCENTESISDokument25 SeitenPERICARDIOCENTESISrastaNoch keine Bewertungen
- Central Venous Pressure Monitoring.: DR Jyothsna Chairperson DR Sunil ChhabriaDokument24 SeitenCentral Venous Pressure Monitoring.: DR Jyothsna Chairperson DR Sunil ChhabriaPriyanka MaiyaNoch keine Bewertungen
- Peripherally Inserted Central CatheterDokument4 SeitenPeripherally Inserted Central CatheterDivine Grace Arreglo AbingNoch keine Bewertungen
- Keck School of Medicine USC Procedural SkillsDokument35 SeitenKeck School of Medicine USC Procedural Skillspuravi91Noch keine Bewertungen
- Radial Artery PunctureDokument6 SeitenRadial Artery Puncturemanalibrahem41Noch keine Bewertungen
- Limba Engleza: Universitatea Bioterra Bucuresti Facultatea de Asistenta Medicala GeneralaDokument3 SeitenLimba Engleza: Universitatea Bioterra Bucuresti Facultatea de Asistenta Medicala GeneralaCristina CrisuNoch keine Bewertungen
- BP - LippincottDokument7 SeitenBP - LippincottForrest LloydNoch keine Bewertungen
- Arterial LinesDokument9 SeitenArterial LinesRei IrincoNoch keine Bewertungen
- Abg AnalysisDokument9 SeitenAbg AnalysisLakshmi RjNoch keine Bewertungen
- CVP MonitoringDokument16 SeitenCVP MonitoringVictor Elvis0% (1)
- Measurement of CENTRAL VENOUS PRESSURE Via A TransducerDokument22 SeitenMeasurement of CENTRAL VENOUS PRESSURE Via A TransducerJasleen KaurNoch keine Bewertungen
- Hemodynamic MonitoringDokument10 SeitenHemodynamic MonitoringDivya Joy100% (1)
- Seminar On Hemodynamic Monitoring: BY UMA Iind Year MSC NursingDokument52 SeitenSeminar On Hemodynamic Monitoring: BY UMA Iind Year MSC NursingAyen AlingNoch keine Bewertungen
- NCM Checklist - Vital SignsDokument18 SeitenNCM Checklist - Vital SignsYanna Habib-Mangotara100% (1)
- ABG Analysis Guide for NursesDokument6 SeitenABG Analysis Guide for NursesSimran Josan100% (4)
- Common Procedures in Paediatric IcuDokument17 SeitenCommon Procedures in Paediatric IcuNeethu Mariya MathewNoch keine Bewertungen
- Hemodynamicmonitorig 160407141401Dokument96 SeitenHemodynamicmonitorig 160407141401abeer alzhoorNoch keine Bewertungen
- Swan GanzDokument35 SeitenSwan Ganzdrivaner1Noch keine Bewertungen
- Procedures ThoracentesisDokument4 SeitenProcedures ThoracentesisPatty MArivel ReinosoNoch keine Bewertungen
- Hemodynamics MonitoringDokument12 SeitenHemodynamics MonitoringBhawna Joshi100% (3)
- IPM NotesDokument4 SeitenIPM NotesPreethi ShekarNoch keine Bewertungen
- Abg 2021-2022Dokument20 SeitenAbg 2021-2022Ahmed AshrafNoch keine Bewertungen
- Arterial LinesDokument13 SeitenArterial LinesYee LengNoch keine Bewertungen
- Hemodialysis Procedure GuideDokument2 SeitenHemodialysis Procedure GuideEdRobertArnad100% (1)
- Ateneo de Zamboanga University College of Nursing NSO on AngiographyDokument5 SeitenAteneo de Zamboanga University College of Nursing NSO on AngiographyLizzey YuNoch keine Bewertungen
- Pulmonary Artery CatheterizationDokument15 SeitenPulmonary Artery Catheterizationأبو أويس شرف الدينNoch keine Bewertungen
- DIAGNOSING HYPERTENSION: BLOOD PRESSURE MEASUREMENT GUIDEDokument37 SeitenDIAGNOSING HYPERTENSION: BLOOD PRESSURE MEASUREMENT GUIDEDhira 'Princess Kalonk' AninditaNoch keine Bewertungen
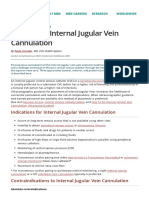
- How To Do Internal Jugular Vein Cannulation - Critical Care Medicine - MSD Manual Professional EditionDokument9 SeitenHow To Do Internal Jugular Vein Cannulation - Critical Care Medicine - MSD Manual Professional EditionnaveenNoch keine Bewertungen
- ABG ProcedureDokument25 SeitenABG ProcedureSophia DimayugaNoch keine Bewertungen
- Final HeartDokument6 SeitenFinal HeartPrincess PlateroNoch keine Bewertungen
- CVP MonitoringDokument7 SeitenCVP Monitoringgurneet kourNoch keine Bewertungen
- CVP Care (Swapnil (Dokument18 SeitenCVP Care (Swapnil (SWAPNIL WANJARINoch keine Bewertungen
- (FEU) Central Venous Pressure Notes PDFDokument25 Seiten(FEU) Central Venous Pressure Notes PDFBryJos tiongsonNoch keine Bewertungen
- Arterial Blood GasDokument55 SeitenArterial Blood GasDharlyn MungcalNoch keine Bewertungen
- Arterial Lines GuideDokument38 SeitenArterial Lines GuideRabeed MohammedNoch keine Bewertungen
- Swan Ganz CatheterizationDokument2 SeitenSwan Ganz CatheterizationJanelle MarceraNoch keine Bewertungen
- Sagar Rathod Pratikshit Raghuwanshi DR.D.D Wagh Dr.P.GhardeDokument46 SeitenSagar Rathod Pratikshit Raghuwanshi DR.D.D Wagh Dr.P.GhardeSagarRathodNoch keine Bewertungen
- CVPNSGDokument19 SeitenCVPNSGmalathiNoch keine Bewertungen
- Hemodynamic MonitoringDokument39 SeitenHemodynamic MonitoringNor Jeannah PolaoNoch keine Bewertungen
- Peran Perawat Di CathlabDokument71 SeitenPeran Perawat Di CathlabMabro CahyoNoch keine Bewertungen
- CVPDokument23 SeitenCVPShalini KaluraNoch keine Bewertungen
- Arterial Lines Mark Hammerschmidt, RN FromDokument9 SeitenArterial Lines Mark Hammerschmidt, RN FromMark Hammerschmidt100% (3)
- CVPDokument25 SeitenCVPNikhil YadavNoch keine Bewertungen
- ABG FinalDokument6 SeitenABG Finalrupali gahalianNoch keine Bewertungen
- Neuromuscular JunctionDokument6 SeitenNeuromuscular JunctionManish GujjarNoch keine Bewertungen
- TRAMADOLDokument4 SeitenTRAMADOLRudie Lee PascualNoch keine Bewertungen
- Patient Data From 1Dokument18 SeitenPatient Data From 1Lalit Surykant ChavanNoch keine Bewertungen
- Biology Unit 5 Review QuestionsDokument9 SeitenBiology Unit 5 Review QuestionsMoa ArmyNoch keine Bewertungen
- Fitness Assessment ManualDokument266 SeitenFitness Assessment ManualVanessa Irene100% (1)
- List of NAAS Scored Journals 2020 - National Academy of Agricultural SciencesDokument67 SeitenList of NAAS Scored Journals 2020 - National Academy of Agricultural SciencesBirjesh YaduvanshiNoch keine Bewertungen
- NCP For HepatitisDokument6 SeitenNCP For Hepatitisorca0767% (3)
- Temperature Regulation & ExerciseDokument41 SeitenTemperature Regulation & ExerciseHidayah HasanNoch keine Bewertungen
- Reymart Baguio A. Iii Bsed-Science Module 4 - Fluids and Transport Module Assessment Critical Thinking QuestionsDokument13 SeitenReymart Baguio A. Iii Bsed-Science Module 4 - Fluids and Transport Module Assessment Critical Thinking QuestionsReymart Anga Baguio IINoch keine Bewertungen
- Heart Railway RPF by Radhika MamDokument70 SeitenHeart Railway RPF by Radhika Mamyakshat.4141ykNoch keine Bewertungen
- Test Bank For Mechanical Ventilation 7th Edition J M CairoDokument11 SeitenTest Bank For Mechanical Ventilation 7th Edition J M CairoJohnCampbellyacer100% (27)
- NCP PediaDokument2 SeitenNCP PediaJoey JoseNoch keine Bewertungen
- Pathophysiology of Cva-Hpnii-Hemorrhagic StrokeDokument2 SeitenPathophysiology of Cva-Hpnii-Hemorrhagic StrokeLarisse de Leon82% (11)
- An Interesting Case of "Trigeminal Tachycardia"Dokument3 SeitenAn Interesting Case of "Trigeminal Tachycardia"ABDULLAH ALHASANNoch keine Bewertungen
- Chapter 2 - Clinical Cardiovascular Examination-2Dokument43 SeitenChapter 2 - Clinical Cardiovascular Examination-2sarahya.medinaNoch keine Bewertungen
- Trionara 06 UM Pac T3 E211128Dokument133 SeitenTrionara 06 UM Pac T3 E211128Rudi CanicelaNoch keine Bewertungen
- Fatime Sanogo Vsim Steps - HTMLDokument6 SeitenFatime Sanogo Vsim Steps - HTMLJhunnieEy ReyesNoch keine Bewertungen
- Kenzo Hirao (Eds.) - Catheter Ablation - A Current Approach On Cardiac Arrhythmias (2018, Springer Singapore) PDFDokument376 SeitenKenzo Hirao (Eds.) - Catheter Ablation - A Current Approach On Cardiac Arrhythmias (2018, Springer Singapore) PDFPanNoch keine Bewertungen
- Receptor TypesDokument3 SeitenReceptor TypesPardeep SonyNoch keine Bewertungen
- Format Laboratorium 4Dokument5 SeitenFormat Laboratorium 4Wahyu Alamsyah DasopangNoch keine Bewertungen
- TISSUES (Prashant Kirad)Dokument9 SeitenTISSUES (Prashant Kirad)abhijotsinghas83Noch keine Bewertungen
- Nursing Board Exam Pointers for SingaporeDokument18 SeitenNursing Board Exam Pointers for SingaporeHegi Ann AlcalaNoch keine Bewertungen
- Arterial Blood Gas AnalysisDokument6 SeitenArterial Blood Gas AnalysisMaribee Tagayun EspirituNoch keine Bewertungen
- Neoreviews 201533Dokument11 SeitenNeoreviews 201533Dmitri KaramazovNoch keine Bewertungen
- Rhythm Control Versus Rate Control For Atrial FibrillationDokument5 SeitenRhythm Control Versus Rate Control For Atrial FibrillationlowellaNoch keine Bewertungen
- Biology O Level Notes PDFDokument36 SeitenBiology O Level Notes PDFGB Hacker100% (1)
- Cardiovascular SystemDokument8 SeitenCardiovascular SystemDawnmurph Dharlene Wag-eNoch keine Bewertungen
- Vincent Brody Care PlanDokument10 SeitenVincent Brody Care PlanKarina Rodriguez50% (2)
- Fluid and Electrolyte Balance LectureDokument16 SeitenFluid and Electrolyte Balance LectureBasa, Rica Mae P.Noch keine Bewertungen
- Chapter 19 - Blood VesselsDokument40 SeitenChapter 19 - Blood VesselsZuleyha ZuleyhaNoch keine Bewertungen