Das könnte Ihnen auch gefallen
- Health and Hatha Yoga by Swami Sivananda CompressDokument356 SeitenHealth and Hatha Yoga by Swami Sivananda CompressLama Fera with Yachna JainNoch keine Bewertungen
- NvsDokument49 SeitenNvsChong Uy AlawiNoch keine Bewertungen
- 5f Time of Legends Joan of Arc RulebookDokument36 Seiten5f Time of Legends Joan of Arc Rulebookpierre borget100% (1)
- Acute GastritisDokument43 SeitenAcute GastritisANCHAL SHARMANoch keine Bewertungen
- CHICKENPOXDokument36 SeitenCHICKENPOXAlyssa Marie Pepito100% (1)
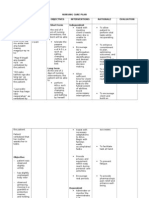
- Nusing CareplanDokument3 SeitenNusing Careplanardec_143Noch keine Bewertungen
- ACFrOgCEv6W8PZIOChX2ac TB PsVqkwB2LLEUA - nz2imEUDlJJqTMiew0fEYsQLz7I hoxDAHunIFV - PnnXqTDHrgpAsGRo2r9aPQF4UMBSoquxza - oenQBKFcGXpRcMCDKlMwgjULOtJeC9idDokument14 SeitenACFrOgCEv6W8PZIOChX2ac TB PsVqkwB2LLEUA - nz2imEUDlJJqTMiew0fEYsQLz7I hoxDAHunIFV - PnnXqTDHrgpAsGRo2r9aPQF4UMBSoquxza - oenQBKFcGXpRcMCDKlMwgjULOtJeC9idCenitserNoch keine Bewertungen
- Concept Map SepsisDokument4 SeitenConcept Map SepsisSavanna ChambersNoch keine Bewertungen
- Barangay AppointmentDokument2 SeitenBarangay AppointmentArlyn Gumahad CahanapNoch keine Bewertungen
- Gastrointestinal System Review of Systems: (Image Taken From Medical-Surgical Nursing, M. Hogan & T. Madayag)Dokument26 SeitenGastrointestinal System Review of Systems: (Image Taken From Medical-Surgical Nursing, M. Hogan & T. Madayag)pawnayNoch keine Bewertungen
- Hankinson - Location Branding - A Study of The Branding Practices of 12 English CitiesDokument16 SeitenHankinson - Location Branding - A Study of The Branding Practices of 12 English CitiesNatalia Ney100% (1)
- Kampfgruppe KerscherDokument6 SeitenKampfgruppe KerscherarkhoshNoch keine Bewertungen
- Hanumaan Bajrang Baan by JDokument104 SeitenHanumaan Bajrang Baan by JAnonymous R8qkzgNoch keine Bewertungen
- Kumar-2011-In Vitro Plant Propagation A ReviewDokument13 SeitenKumar-2011-In Vitro Plant Propagation A ReviewJuanmanuelNoch keine Bewertungen
- Nursing Care Plan: Fluid Volume Deficit R/T Active Fluid Loss (Increased Urine Output)Dokument9 SeitenNursing Care Plan: Fluid Volume Deficit R/T Active Fluid Loss (Increased Urine Output)Gayu Patel0% (1)
- Management of Tuberculosis: A guide for clinicians (eBook edition)Von EverandManagement of Tuberculosis: A guide for clinicians (eBook edition)Noch keine Bewertungen
- Chapter 16 - Test Bank Chem 200Dokument110 SeitenChapter 16 - Test Bank Chem 200Jan Chester Chan80% (5)
- Case AnalysisDokument25 SeitenCase AnalysisGerly LagutingNoch keine Bewertungen
- Nursing Care PlanDokument26 SeitenNursing Care PlanDinda MaretaNoch keine Bewertungen
- NCP QuizonDokument2 SeitenNCP QuizonChe ValenzuelaNoch keine Bewertungen
- 1 Ineffective Peripheral Tissue PerfusionDokument1 Seite1 Ineffective Peripheral Tissue Perfusionjean_fabulaNoch keine Bewertungen
- GIT DiSEASES Dumping SyndromeDokument3 SeitenGIT DiSEASES Dumping SyndromeLheidaniel MMM.Noch keine Bewertungen
- Pigeon Racing PigeonDokument7 SeitenPigeon Racing Pigeonsundarhicet83Noch keine Bewertungen
- 5g-core-guide-building-a-new-world Переход от лте к 5г английскийDokument13 Seiten5g-core-guide-building-a-new-world Переход от лте к 5г английскийmashaNoch keine Bewertungen
- Ba GastrectomyDokument10 SeitenBa GastrectomyHope3750% (2)
- CholecystitisDokument12 SeitenCholecystitisMariela HuertaNoch keine Bewertungen
- Self Care DeficitDokument3 SeitenSelf Care DeficitChristy BerryNoch keine Bewertungen
- Pediatric Appendicitis Clinical Presentation - History, Physical ExaminationDokument5 SeitenPediatric Appendicitis Clinical Presentation - History, Physical ExaminationBayu Surya DanaNoch keine Bewertungen
- Dengue Hemorrhagic FeverDokument9 SeitenDengue Hemorrhagic FevermarianegvNoch keine Bewertungen
- Week 7 - Rheumatoid ArthritisDokument1 SeiteWeek 7 - Rheumatoid ArthritisTuTitNoch keine Bewertungen
- NCP Gastric CancerDokument7 SeitenNCP Gastric CancerHilario. Hayascent.Reign.M.Noch keine Bewertungen
- 51 100Dokument18 Seiten51 100Jaessa Feliciano100% (1)
- Avian Influenza: You May Have QuestionsDokument18 SeitenAvian Influenza: You May Have QuestionsФарзана ЙусуфNoch keine Bewertungen
- Fluid and Electrolytes, Burns, G.UDokument56 SeitenFluid and Electrolytes, Burns, G.Uapi-3735995100% (4)
- Pontine BleedingDokument99 SeitenPontine BleedingJeffrey Dela CruzNoch keine Bewertungen
- CiprofloxacinDokument1 SeiteCiprofloxacindwightciderNoch keine Bewertungen
- Assessment Diagnosis Planning Implementation Evaluation Goal: Intervention: Independent: Rationale: The Goal MetDokument2 SeitenAssessment Diagnosis Planning Implementation Evaluation Goal: Intervention: Independent: Rationale: The Goal MetJulie AnnNoch keine Bewertungen
- Patient ChartDokument2 SeitenPatient ChartHydieNoch keine Bewertungen
- Patient's Name: Medical Diagnosis: LBM, Vomiting, Fever Age: 1year Old Gender: MaleDokument3 SeitenPatient's Name: Medical Diagnosis: LBM, Vomiting, Fever Age: 1year Old Gender: MaleIsan LutzNoch keine Bewertungen
- Chapter 1 Fundamental Concepts SPSS - Descriptive StatisticsDokument4 SeitenChapter 1 Fundamental Concepts SPSS - Descriptive StatisticsAvinash AmbatiNoch keine Bewertungen
- GRP 4 CLO 2 Concept Map PT 1 PDFDokument14 SeitenGRP 4 CLO 2 Concept Map PT 1 PDFMaria Lyn Ocariza ArandiaNoch keine Bewertungen
- Meniere's Disease - Case StudyDokument3 SeitenMeniere's Disease - Case StudyZORANASNNoch keine Bewertungen
- Drug Study TramadolDokument1 SeiteDrug Study Tramadolpius troy macapazNoch keine Bewertungen
- Acute and Chronic GastritisDokument6 SeitenAcute and Chronic GastritisAnn CanNoch keine Bewertungen
- Acute and Chronic PyelonephritisDokument7 SeitenAcute and Chronic PyelonephritisMatthew Ryan100% (1)
- CTStudy QuestionsDokument2 SeitenCTStudy Questionsjaijai magbanuaNoch keine Bewertungen
- Nursing Care Plan Impaired Gas ExchangeDokument1 SeiteNursing Care Plan Impaired Gas ExchangeKarylle PetilNoch keine Bewertungen
- NCP BronchopneumoniaDokument8 SeitenNCP BronchopneumoniaCrisantaCasliNoch keine Bewertungen
- Atropine: Drug Study: NCM 106 PharmacologyDokument6 SeitenAtropine: Drug Study: NCM 106 PharmacologyKevin RosalesNoch keine Bewertungen
- Health Assessment 51-100 QuestionnaireDokument27 SeitenHealth Assessment 51-100 QuestionnairetflorenzNoch keine Bewertungen
- Nursing Diagnosis - Saliva Test For HIVDokument3 SeitenNursing Diagnosis - Saliva Test For HIVMarsha AngelieNoch keine Bewertungen
- Liver Cirrhosis Care PlanDokument3 SeitenLiver Cirrhosis Care PlanWendy EscalanteNoch keine Bewertungen
- Moira Mae B. Balite BSN 2A: Post Partum Care DefinitionDokument5 SeitenMoira Mae B. Balite BSN 2A: Post Partum Care DefinitionMoiraMaeBeridoBaliteNoch keine Bewertungen
- NCPDokument2 SeitenNCPMelissa David100% (1)
- Ineffective Peripheral Tissue Perfusion Related To Vasoconstriction Secondary To High Glucose Level.Dokument6 SeitenIneffective Peripheral Tissue Perfusion Related To Vasoconstriction Secondary To High Glucose Level.SAROL, RYAN CHRISTIAN B.Noch keine Bewertungen
- Ranitidine, ParacetamolDokument3 SeitenRanitidine, ParacetamoltaekadoNoch keine Bewertungen
- TrihexyphenidylDokument5 SeitenTrihexyphenidylZepHemaNoch keine Bewertungen
- Basic Concepts in NursingDokument9 SeitenBasic Concepts in NursingLilian FloresNoch keine Bewertungen
- Care of Pediatric Client With Dermatologic DisorderDokument3 SeitenCare of Pediatric Client With Dermatologic DisorderAraw GabiNoch keine Bewertungen
- Nursing Care PlanDokument4 SeitenNursing Care PlanDewi PurnamasariNoch keine Bewertungen
- Kardex: Mental Status - Conscious Activities Diet Tubes Special InfoDokument6 SeitenKardex: Mental Status - Conscious Activities Diet Tubes Special InfoCaitlynNoch keine Bewertungen
- Clinical PaperDokument18 SeitenClinical PaperlhhjklllNoch keine Bewertungen
- Atun Maricris Jorre Ca2 Au Legarda Leadership Managemet Research DownloadableDokument2 SeitenAtun Maricris Jorre Ca2 Au Legarda Leadership Managemet Research DownloadableCharissa Magistrado De LeonNoch keine Bewertungen
- NCP PainDokument2 SeitenNCP PainApril_Ivy_Raga_3835Noch keine Bewertungen
- NCP Bed SoresDokument3 SeitenNCP Bed SoresShe CalliNoch keine Bewertungen
- Introduction To Community Health and Environmental Sanitation PDFDokument44 SeitenIntroduction To Community Health and Environmental Sanitation PDFKaty SanchezNoch keine Bewertungen
- Patient C.J.S: Gasping of Air Not Responding Verbal StimuliDokument3 SeitenPatient C.J.S: Gasping of Air Not Responding Verbal StimuliJasmin B. ERMITANoch keine Bewertungen
- Intracranial HemorrhageDokument41 SeitenIntracranial Hemorrhagedoctormussieaberra100% (1)
- 6 Nursing Care Plan 1Dokument2 Seiten6 Nursing Care Plan 1Denise Louise PoNoch keine Bewertungen
- Pemicu 3 GIT BudiDokument67 SeitenPemicu 3 GIT BudiGrace KahonoNoch keine Bewertungen
- The Nature of Mathematics: "Nature's Great Books Is Written in Mathematics" Galileo GalileiDokument9 SeitenThe Nature of Mathematics: "Nature's Great Books Is Written in Mathematics" Galileo GalileiLei-Angelika TungpalanNoch keine Bewertungen
- Oral Oncology: Jingyi Liu, Yixiang DuanDokument9 SeitenOral Oncology: Jingyi Liu, Yixiang DuanSabiran GibranNoch keine Bewertungen
- A List of Run Commands For Wind - Sem AutorDokument6 SeitenA List of Run Commands For Wind - Sem AutorJoão José SantosNoch keine Bewertungen
- 2 Lista Total de Soportados 14-12-2022Dokument758 Seiten2 Lista Total de Soportados 14-12-2022Emanuel EspindolaNoch keine Bewertungen
- Georgia Jean Weckler 070217Dokument223 SeitenGeorgia Jean Weckler 070217api-290747380Noch keine Bewertungen
- PropertycasesforfinalsDokument40 SeitenPropertycasesforfinalsRyan Christian LuposNoch keine Bewertungen
- Precertification Worksheet: LEED v4.1 BD+C - PrecertificationDokument62 SeitenPrecertification Worksheet: LEED v4.1 BD+C - PrecertificationLipi AgarwalNoch keine Bewertungen
- New Kanban System DesignDokument4 SeitenNew Kanban System DesignJebin GeorgeNoch keine Bewertungen
- Ob AssignmntDokument4 SeitenOb AssignmntOwais AliNoch keine Bewertungen
- Cryptography Practical 1Dokument41 SeitenCryptography Practical 1Harsha GangwaniNoch keine Bewertungen
- ch-1 NewDokument11 Seitench-1 NewSAKIB MD SHAFIUDDINNoch keine Bewertungen
- Amt 3103 - Prelim - Module 1Dokument17 SeitenAmt 3103 - Prelim - Module 1kim shinNoch keine Bewertungen
- Brahm Dutt v. UoiDokument3 SeitenBrahm Dutt v. Uoiswati mohapatraNoch keine Bewertungen
- ANI Network - Quick Bill Pay PDFDokument2 SeitenANI Network - Quick Bill Pay PDFSandeep DwivediNoch keine Bewertungen
- Jewish Standard, September 16, 2016Dokument72 SeitenJewish Standard, September 16, 2016New Jersey Jewish StandardNoch keine Bewertungen
- Pharmaniaga Paracetamol Tablet: What Is in This LeafletDokument2 SeitenPharmaniaga Paracetamol Tablet: What Is in This LeafletWei HangNoch keine Bewertungen
- Name: Nur Hashikin Binti Ramly (2019170773) Course Code: Udm713 - Decision Making Methods and Analysis Assignment Title: Need Gap AnalysisDokument2 SeitenName: Nur Hashikin Binti Ramly (2019170773) Course Code: Udm713 - Decision Making Methods and Analysis Assignment Title: Need Gap AnalysisAhmad HafizNoch keine Bewertungen
- Cat Hydo 10wDokument4 SeitenCat Hydo 10wWilbort Encomenderos RuizNoch keine Bewertungen
- BSBHRM405 Support Recruitment, Selection and Induction of Staff KM2Dokument17 SeitenBSBHRM405 Support Recruitment, Selection and Induction of Staff KM2cplerkNoch keine Bewertungen
- Assignment File - Group PresentationDokument13 SeitenAssignment File - Group PresentationSAI NARASIMHULUNoch keine Bewertungen