Das könnte Ihnen auch gefallen
- Anti Malaria Agent: Novrita PadaulengDokument23 SeitenAnti Malaria Agent: Novrita PadaulengMuhammad Bilal Bin AmirNoch keine Bewertungen
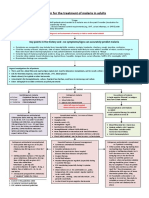
- Algorithm For The Treatment of Malaria in AdultsDokument1 SeiteAlgorithm For The Treatment of Malaria in AdultsRihab IsmaeelNoch keine Bewertungen
- Elsye Gunawan: Farmakoterapi Pada Pasien MalariaDokument47 SeitenElsye Gunawan: Farmakoterapi Pada Pasien MalariaEnvhy WinaNoch keine Bewertungen
- Malaria 2012Dokument43 SeitenMalaria 2012van_cristianoNoch keine Bewertungen
- Afb5 - 1. Antimalarials MedicalDokument63 SeitenAfb5 - 1. Antimalarials MedicalAx D98Noch keine Bewertungen
- Pharmacology-Unit-III (F) AntimalarialdrugsDokument59 SeitenPharmacology-Unit-III (F) Antimalarialdrugswebpixel services100% (1)
- Malaria ChemotherapyDokument74 SeitenMalaria ChemotherapyGeorge C. KasondaNoch keine Bewertungen
- MalariaDokument30 SeitenMalariaRevan NasirNoch keine Bewertungen
- Antimalarial Drugs Review - TaggedDokument29 SeitenAntimalarial Drugs Review - Taggeddagehi6880Noch keine Bewertungen
- Acute Pyelonephritis Treatment & Management: Approach ConsiderationsDokument4 SeitenAcute Pyelonephritis Treatment & Management: Approach ConsiderationsPeter InocandoNoch keine Bewertungen
- Classification (S) Therapeutic: Anti-Infectives Pharmacologic: FluoroquinolonesDokument9 SeitenClassification (S) Therapeutic: Anti-Infectives Pharmacologic: FluoroquinolonesFildehl Janice Bomediano CatipayNoch keine Bewertungen
- Esbl Producing eDokument45 SeitenEsbl Producing eapi-205355237Noch keine Bewertungen
- Drugs Related To ClottingDokument23 SeitenDrugs Related To ClottingBig PigNoch keine Bewertungen
- Envenomation and IntoxicationDokument37 SeitenEnvenomation and IntoxicationYoelBagusGiartoNoch keine Bewertungen
- ANTIMALARIAL DrugsDokument25 SeitenANTIMALARIAL DrugsMANAS ChhapoliyaNoch keine Bewertungen
- Anti MalariaDokument49 SeitenAnti MalariaYIKI ISAACNoch keine Bewertungen
- 7 - Case - ParasiticDokument18 Seiten7 - Case - Parasitickoteshwara raoNoch keine Bewertungen
- Antimalarial DrugsDokument56 SeitenAntimalarial DrugsKasturiRangan SrivatsaNoch keine Bewertungen
- Anti Malarial Drugs by Salaria AnamikaDokument10 SeitenAnti Malarial Drugs by Salaria AnamikaSalaria Anamika100% (1)
- Malaria: DR MD Mamunul Abedin ShimulDokument41 SeitenMalaria: DR MD Mamunul Abedin ShimulDr. Mamunul AbedinNoch keine Bewertungen
- Pharmacology of AntimalarialsDokument39 SeitenPharmacology of AntimalarialsAntonyNoch keine Bewertungen
- Am Pic Ill InsDokument4 SeitenAm Pic Ill Insapi-3797941Noch keine Bewertungen
- Malaria MB CHB January 2018-FinalDokument36 SeitenMalaria MB CHB January 2018-Finalokwadha simionNoch keine Bewertungen
- Antiprotozoal Antimalarial DrugsDokument49 SeitenAntiprotozoal Antimalarial DrugsFredericka QuayeNoch keine Bewertungen
- Neutropenic Sepsis-Tls-Anaphylaxis-ExtravasationDokument40 SeitenNeutropenic Sepsis-Tls-Anaphylaxis-ExtravasationSA NodeNoch keine Bewertungen
- MALARIADokument36 SeitenMALARIAMutegeki AdolfNoch keine Bewertungen
- MalariaDokument44 SeitenMalariasantosh goitNoch keine Bewertungen
- Malaria: Dr. Harun Hudari, SPPDDokument49 SeitenMalaria: Dr. Harun Hudari, SPPDEdvans HenryNoch keine Bewertungen
- FluconazoleDokument3 SeitenFluconazoleapi-3797941100% (1)
- Drugs Study of Omeprazole, Metoclopramide EtcDokument12 SeitenDrugs Study of Omeprazole, Metoclopramide EtcMargaret Cortinas75% (4)
- UtiDokument28 SeitenUtiDrShweta SainiNoch keine Bewertungen
- Cirrhosis With SBPDokument22 SeitenCirrhosis With SBPapi-648401824Noch keine Bewertungen
- Antibiotik Dan Antiseptik Saluran KemihDokument29 SeitenAntibiotik Dan Antiseptik Saluran KemihPutri Sari SeptirianiNoch keine Bewertungen
- Management of MalariaDokument55 SeitenManagement of MalariaAnu SinhaNoch keine Bewertungen
- 08 Complicated MalariaDokument36 Seiten08 Complicated MalariaMwanja MosesNoch keine Bewertungen
- Hypertensive Disorders of Pregnancy: Dr. Dianne MP Graham, MD, CCFPDokument28 SeitenHypertensive Disorders of Pregnancy: Dr. Dianne MP Graham, MD, CCFPNinaNoch keine Bewertungen
- Ciprofloxacin (Drug Study)Dokument3 SeitenCiprofloxacin (Drug Study)Franz.thenurse6888Noch keine Bewertungen
- Tropmed MANTAP StudentDokument72 SeitenTropmed MANTAP StudentMorindaNoch keine Bewertungen
- En Ox A Par inDokument3 SeitenEn Ox A Par inapi-3797941Noch keine Bewertungen
- Receiving Concurrent Moderate CYP3A4 Inhibitors (Erythromycin, Saquinavir, Verapamil, Fluconazole) - 25 MG Once Daily InitiallyDokument272 SeitenReceiving Concurrent Moderate CYP3A4 Inhibitors (Erythromycin, Saquinavir, Verapamil, Fluconazole) - 25 MG Once Daily InitiallyFatima Doran PandaogNoch keine Bewertungen
- Tungul - Activity 1 Midterms (Pharmacology)Dokument6 SeitenTungul - Activity 1 Midterms (Pharmacology)Ma. Rita Concepcion TungulNoch keine Bewertungen
- 12 MalariaDokument61 Seiten12 MalariaMewael TesfamichaelNoch keine Bewertungen
- Acute Pancreatitis, HemakshiDokument25 SeitenAcute Pancreatitis, HemakshiUmair FirdousNoch keine Bewertungen
- LevofloxacinDokument3 SeitenLevofloxacinapi-3797941100% (2)
- Antiparasitic Agents RevisedDokument94 SeitenAntiparasitic Agents RevisedJe SantosNoch keine Bewertungen
- Guidelines For First-Line Empirical Antibiotic Therapy in AdultsDokument1 SeiteGuidelines For First-Line Empirical Antibiotic Therapy in AdultsAnonymous s4yarxNoch keine Bewertungen
- Antibiotka PicuDokument4 SeitenAntibiotka Picusunu rachmat100% (1)
- Sepsis and Septic Shock Management Guidelines 2019: Insp. Dr. Sunder Chapagain Nepal APF Hospital KathmanduDokument33 SeitenSepsis and Septic Shock Management Guidelines 2019: Insp. Dr. Sunder Chapagain Nepal APF Hospital KathmanduKHAIRUL REDZUANNoch keine Bewertungen
- CiprofloxacinDokument3 SeitenCiprofloxacinapi-3797941Noch keine Bewertungen
- Amikacin SulfateDokument4 SeitenAmikacin SulfateCay SevillaNoch keine Bewertungen
- Anti Malarial DrugsDokument42 SeitenAnti Malarial DrugsSaurabh GautamNoch keine Bewertungen
- Farmakologi Obat AntikoagulanDokument20 SeitenFarmakologi Obat AntikoagulanHenderi SaputraNoch keine Bewertungen
- Sine Derivates IM Versus Quinine IV in TreatmentDokument18 SeitenSine Derivates IM Versus Quinine IV in TreatmentNiek VersteegdeNoch keine Bewertungen
- Basic Pharmacology: NTA Level 4 Semester 2Dokument23 SeitenBasic Pharmacology: NTA Level 4 Semester 2MabusiNoch keine Bewertungen
- Farmakoterapi Pada SepsisDokument36 SeitenFarmakoterapi Pada SepsisNathaniaNoch keine Bewertungen
- Leptospirosis Case Study (Short)Dokument16 SeitenLeptospirosis Case Study (Short)Liryc Ernest CuerboNoch keine Bewertungen
- Medicine RotatationbookletDokument20 SeitenMedicine RotatationbookletJanelle JosephsNoch keine Bewertungen
- Drug StudyDokument16 SeitenDrug StudyJhann0% (1)
- Dengue FinalDokument44 SeitenDengue FinalAniket MuleNoch keine Bewertungen
- Airway ObstructionDokument13 SeitenAirway ObstructionBaiqLinaAnggrianNoch keine Bewertungen
- BronchiectasisDokument17 SeitenBronchiectasisBaiqLinaAnggrianNoch keine Bewertungen
- Kuliah Antihelmintic DrugsDokument23 SeitenKuliah Antihelmintic DrugsBaiqLinaAnggrianNoch keine Bewertungen
- Antifungal Agents: Halia Wanadiatri, DR., M.SiDokument24 SeitenAntifungal Agents: Halia Wanadiatri, DR., M.SiBaiqLinaAnggrianNoch keine Bewertungen
- Fakultas Kedokteran Universitas Islam Al Azhar: Dr. Dasti Anditiarina, SP - KPDokument30 SeitenFakultas Kedokteran Universitas Islam Al Azhar: Dr. Dasti Anditiarina, SP - KPBaiqLinaAnggrianNoch keine Bewertungen
- Soft-Tissue Tumors and Tumor-Like Lesions: Dr. I Made Naris Pujawan, M.Biomed, SP - PADokument17 SeitenSoft-Tissue Tumors and Tumor-Like Lesions: Dr. I Made Naris Pujawan, M.Biomed, SP - PABaiqLinaAnggrianNoch keine Bewertungen
- 2 Benign Lesions of BoneDokument28 Seiten2 Benign Lesions of BoneBaiqLinaAnggrianNoch keine Bewertungen
- 1 STROKE Kuliah UnizarDokument52 Seiten1 STROKE Kuliah UnizarBaiqLinaAnggrianNoch keine Bewertungen
- Chronic Kidney Disease LIFA FixxxDokument19 SeitenChronic Kidney Disease LIFA FixxxMuzdalifa MohamadNoch keine Bewertungen
- EPI Schedule Malawi COM 2017Dokument2 SeitenEPI Schedule Malawi COM 2017INNOCENT KHULIWANoch keine Bewertungen
- McqepilipsyDokument3 SeitenMcqepilipsyNguyen Anh TuanNoch keine Bewertungen
- Antibiotic ChartsDokument61 SeitenAntibiotic Chartspempekplg100% (1)
- Miasms Chart - PDF VersionDokument1 SeiteMiasms Chart - PDF Versionsergiomiguelgomes992369% (16)
- PreeclampsiaDokument9 SeitenPreeclampsiaBhawna Sharma67% (3)
- Format Rko Program 2020Dokument18 SeitenFormat Rko Program 2020Anonymous ItXYBoaC1CNoch keine Bewertungen
- DermatologytherapyDokument642 SeitenDermatologytherapyDhyna MutiarasariNoch keine Bewertungen
- PPS CPG UtiDokument8 SeitenPPS CPG UtiPaula QuiñonesNoch keine Bewertungen
- Abdominal Pain - Royal Children HospitalDokument4 SeitenAbdominal Pain - Royal Children HospitalMehrdad IraniNoch keine Bewertungen
- Bavshvta Kardiologia 2009 PDFDokument64 SeitenBavshvta Kardiologia 2009 PDFDimitri KochadzeNoch keine Bewertungen
- Medication: Expected Pharmacological Action Therapeutic UseDokument1 SeiteMedication: Expected Pharmacological Action Therapeutic UseMike EveretteNoch keine Bewertungen
- GHE2015 Deaths Global 2000 2015Dokument42 SeitenGHE2015 Deaths Global 2000 2015mikeNoch keine Bewertungen
- Spina BifidaDokument12 SeitenSpina Bifidasalsabil aurellNoch keine Bewertungen
- PGB 2 - Parte IiDokument32 SeitenPGB 2 - Parte Iikira1234Noch keine Bewertungen
- Hydroxychloroquine PELDokument3 SeitenHydroxychloroquine PELscribd_deepak100% (1)
- Lumpy Jaw in WallabiesDokument6 SeitenLumpy Jaw in WallabiesO'il RuangNoch keine Bewertungen
- Balbas Pusa Scientific NameDokument6 SeitenBalbas Pusa Scientific NameJay-Anne BarbadoNoch keine Bewertungen
- Stock AbstractDokument113 SeitenStock AbstractsriramNoch keine Bewertungen
- Signs and Symptoms: Kawasaki DiseaseDokument6 SeitenSigns and Symptoms: Kawasaki DiseaseBhebe Ocela PanizaNoch keine Bewertungen
- Co Amoxiclav (Broad Spectrum Penicillin)Dokument3 SeitenCo Amoxiclav (Broad Spectrum Penicillin)Danielle Marie SamblacenoNoch keine Bewertungen
- Pharmacology Antibiotics: Fluoroquinolone - Chloramphenicol - TetracycllineDokument40 SeitenPharmacology Antibiotics: Fluoroquinolone - Chloramphenicol - TetracycllinemluthfidunandNoch keine Bewertungen
- The Science of HCC Documentation and CodingDokument20 SeitenThe Science of HCC Documentation and Codingvaish786Noch keine Bewertungen
- Medicine History and CounsellingDokument13 SeitenMedicine History and Counsellingpranjl100% (1)
- Tugas MedicineDokument2 SeitenTugas MedicineRiza Ikhsan MuliaNoch keine Bewertungen
- Faktor-Faktor Yang Berhubungan Dengan Kejadian Dermatitis Atopik Di Puskesmas Bangkinang KotaDokument10 SeitenFaktor-Faktor Yang Berhubungan Dengan Kejadian Dermatitis Atopik Di Puskesmas Bangkinang KotaAsha NopatiNoch keine Bewertungen
- ImmunizationDokument2 SeitenImmunizationannamcconkeyNoch keine Bewertungen
- Daftar Obat Klinik Rumah SehatDokument11 SeitenDaftar Obat Klinik Rumah SehatDr OkialfinNoch keine Bewertungen
- Pediatrics Station Name DateDokument12 SeitenPediatrics Station Name DateSayar GyiNoch keine Bewertungen
- HPV Lay LectureDokument32 SeitenHPV Lay LectureGene LynNoch keine Bewertungen