Das könnte Ihnen auch gefallen
- Tongue and Its MusculatureDokument89 SeitenTongue and Its MusculaturedrsanketcNoch keine Bewertungen
- Dr. Peter McCullough - COVID Vaccines Have Already Killed 50,000 Americans.Dokument7 SeitenDr. Peter McCullough - COVID Vaccines Have Already Killed 50,000 Americans.chingatchgook80% (5)
- A Simple Guide to The Laryngitis and Vocal Cord DiseasesVon EverandA Simple Guide to The Laryngitis and Vocal Cord DiseasesNoch keine Bewertungen
- TONGUEDokument63 SeitenTONGUEAthulya LakshmananNoch keine Bewertungen
- Uterine CancerDokument20 SeitenUterine Cancerzyrine jhen100% (4)
- Monthly Wellness Tip Heat StressDokument1 SeiteMonthly Wellness Tip Heat StressbharathaninNoch keine Bewertungen
- Digestive System of The FrogDokument73 SeitenDigestive System of The FrogNi Ki TaNoch keine Bewertungen
- Caroline Stone. Osteopathic ApproachDokument54 SeitenCaroline Stone. Osteopathic ApproachIoan Andra100% (5)
- Anatomy and Physiology of Normal DeglutitionDokument49 SeitenAnatomy and Physiology of Normal Deglutitionapi-295418186Noch keine Bewertungen
- Anatomy of AirwaysDokument6 SeitenAnatomy of Airwaysgdubs215Noch keine Bewertungen
- Basic and Compulsory Registration of 2004 2016Dokument27 SeitenBasic and Compulsory Registration of 2004 2016BA Ong50% (4)
- Dental Caries IndexDokument35 SeitenDental Caries Indexdr parveen bathla100% (1)
- Mci Ayn Muswil PtbmmkiDokument49 SeitenMci Ayn Muswil PtbmmkiLucya WulandariNoch keine Bewertungen
- ThesisDokument30 SeitenThesisSimran JosanNoch keine Bewertungen
- Pemicu 1 DessyDokument184 SeitenPemicu 1 DessyDessy DsyNoch keine Bewertungen
- Pemicu 1 GI GraceDokument146 SeitenPemicu 1 GI Gracegrace liwantoNoch keine Bewertungen
- Digestive SystemDokument5 SeitenDigestive SystemchipsNoch keine Bewertungen
- GIT-Pemicu 1: Rachelle Betsy - 405140052Dokument149 SeitenGIT-Pemicu 1: Rachelle Betsy - 405140052Michelle Betsy AliantoNoch keine Bewertungen
- Oral CavityDokument20 SeitenOral CavityadileidalaaNoch keine Bewertungen
- W2-8 Oral Region Lecture PDFDokument69 SeitenW2-8 Oral Region Lecture PDFSAHIL AGARWALNoch keine Bewertungen
- Anatomy of Physiology of Swallowing PDFDokument121 SeitenAnatomy of Physiology of Swallowing PDFSaad SayedurNoch keine Bewertungen
- The Digestive SystemDokument41 SeitenThe Digestive Systemkrmgxc8p4fNoch keine Bewertungen
- Anatomy and Physiology of The Digestive System: Dipali HarkhaniDokument83 SeitenAnatomy and Physiology of The Digestive System: Dipali HarkhaniPatel archiNoch keine Bewertungen
- L. 10 The Oral CavityDokument79 SeitenL. 10 The Oral CavityAsfoor gake1Noch keine Bewertungen
- GIT Anatomy Learning ObjectivesDokument5 SeitenGIT Anatomy Learning ObjectivesangrypandasaredangerousNoch keine Bewertungen
- Pemicu 1 Blok Gatrointestinal Kelompok 3Dokument119 SeitenPemicu 1 Blok Gatrointestinal Kelompok 3Steven Junius ChandraNoch keine Bewertungen
- Unit 5 Digestive SystemDokument86 SeitenUnit 5 Digestive SystemPetrus HeinrichNoch keine Bewertungen
- Dzuhri Al Okta: 405140187 Pemicu 1 GIDokument29 SeitenDzuhri Al Okta: 405140187 Pemicu 1 GIjesslynNoch keine Bewertungen
- Bahan Pemicu 1 Gastrointestinal Ivan BuntaraDokument151 SeitenBahan Pemicu 1 Gastrointestinal Ivan BuntaraMarco GunawanNoch keine Bewertungen
- SwallowingDokument44 SeitenSwallowingq4cyfv8t8nNoch keine Bewertungen
- Accessory Organs of The Git - Gross AnatomyDokument172 SeitenAccessory Organs of The Git - Gross AnatomyManisha RaoNoch keine Bewertungen
- Digestive System Part 1Dokument38 SeitenDigestive System Part 1mozajamil777Noch keine Bewertungen
- Anatomy of The Oral CavityDokument56 SeitenAnatomy of The Oral CavitySaidu TanimuNoch keine Bewertungen
- Anatomi Digestif Dr. TaraDokument35 SeitenAnatomi Digestif Dr. TaraAnnisa SafiraNoch keine Bewertungen
- Digestive Anatomy of AnimalsDokument336 SeitenDigestive Anatomy of AnimalsTatenda MagejaNoch keine Bewertungen
- Anatomy 2nd-U-4 Digestive SystemDokument176 SeitenAnatomy 2nd-U-4 Digestive Systemsinte beyuNoch keine Bewertungen
- Lecture 12Dokument7 SeitenLecture 12rahaf alshoumaryNoch keine Bewertungen
- Chapter XI DigestiveDokument19 SeitenChapter XI DigestiveTitoMacoyTVNoch keine Bewertungen
- RT Basics Digestive SystemDokument88 SeitenRT Basics Digestive Systemmaricar paracadNoch keine Bewertungen
- Digestive SystemDokument10 SeitenDigestive SystemElyka Alivan Valdez PolonioNoch keine Bewertungen
- Anatomy and Physiology of The Digestive SystemDokument77 SeitenAnatomy and Physiology of The Digestive SystemWhat do you want?Noch keine Bewertungen
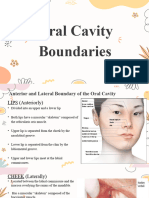
- Oral Cavity BoundariesDokument8 SeitenOral Cavity BoundariesLean Edrielle BillonesNoch keine Bewertungen
- Anatomy of The Upper DigestionDokument16 SeitenAnatomy of The Upper DigestionNabilla MahyendaNoch keine Bewertungen
- EssaysDokument176 SeitenEssaysppdzssx7ghNoch keine Bewertungen
- Oral RegionDokument40 SeitenOral RegionDayen LimNoch keine Bewertungen
- Lect. 12 Digestive SystemDokument74 SeitenLect. 12 Digestive Systemflex gyNoch keine Bewertungen
- Pemicu 1 GIT Aldi FDokument86 SeitenPemicu 1 GIT Aldi Faldi firdausNoch keine Bewertungen
- Digestive System - : Anatomy-Physiology Including Liver, Pancreas Diseases: Peptic Ulcers, HepatitisDokument73 SeitenDigestive System - : Anatomy-Physiology Including Liver, Pancreas Diseases: Peptic Ulcers, Hepatitistanmay mehtaNoch keine Bewertungen
- Kuliah DNMDokument30 SeitenKuliah DNMpunthadewaNoch keine Bewertungen
- BY Tim Anatomi FKG UPDM (B) DRG Theresia Suhartati PAK DR Andy Hidayat M.Biomed Drg. Pricillia Priska Sianita M.Kes.,Sp - OrtDokument34 SeitenBY Tim Anatomi FKG UPDM (B) DRG Theresia Suhartati PAK DR Andy Hidayat M.Biomed Drg. Pricillia Priska Sianita M.Kes.,Sp - OrtFMLNoch keine Bewertungen
- Swallowing 47Dokument48 SeitenSwallowing 47Ju Ju WareeratNoch keine Bewertungen
- Dental Physiology: DR - Shawfekar Bte HJ Abdul HamidDokument77 SeitenDental Physiology: DR - Shawfekar Bte HJ Abdul HamidplsssssNoch keine Bewertungen
- Fernando Oral Cavity AnatomyDokument57 SeitenFernando Oral Cavity AnatomyPatNoch keine Bewertungen
- Oral Cavity Hard & Soft Palate: Dr. Bashir Ahmed ShaikhDokument19 SeitenOral Cavity Hard & Soft Palate: Dr. Bashir Ahmed ShaikhHamza IqbalNoch keine Bewertungen
- 14-ORAL CAVITY and Pharynx FinalDokument50 Seiten14-ORAL CAVITY and Pharynx FinalSudeep DhakalNoch keine Bewertungen
- ANATOMY ORAL CAVITY and TONGUE JelDokument54 SeitenANATOMY ORAL CAVITY and TONGUE JelCoy EnNoch keine Bewertungen
- UNIT - 9 Digestive SystemDokument187 SeitenUNIT - 9 Digestive SystemChandan ShahNoch keine Bewertungen
- Digestive System of Human (Biology)Dokument35 SeitenDigestive System of Human (Biology)liofve X viNoch keine Bewertungen
- Anatomy Histology of The Oral Cavity2 3Dokument31 SeitenAnatomy Histology of The Oral Cavity2 3drsondosNoch keine Bewertungen
- Pemicu 1 GI: Mustika Rukmana 405130182 Kel 1Dokument69 SeitenPemicu 1 GI: Mustika Rukmana 405130182 Kel 1tikaNoch keine Bewertungen
- Digestive LectureDokument20 SeitenDigestive LectureKyla Mae ZabalaNoch keine Bewertungen
- Problem 1Dokument111 SeitenProblem 1Agustina CynthiaNoch keine Bewertungen
- TONGUE Seminar by MeDokument84 SeitenTONGUE Seminar by MeArpita SankhwarNoch keine Bewertungen
- Digestive SystemDokument44 SeitenDigestive SystemMekdelawit AyeleNoch keine Bewertungen
- Digestive SystemDokument64 SeitenDigestive SystemAyro Business CenterNoch keine Bewertungen
- Digestive SystemDokument9 SeitenDigestive System79ctq9xpf7Noch keine Bewertungen
- Digestive SystemDokument121 SeitenDigestive SystemdearnibNoch keine Bewertungen
- The MouthDokument16 SeitenThe MouthNiño GarciaNoch keine Bewertungen
- Pemicu 4 GastroDokument78 SeitenPemicu 4 GastroMudita DewiNoch keine Bewertungen
- Corneal SignDokument6 SeitenCorneal SignMudita DewiNoch keine Bewertungen
- Arianto Salim - Pemicu 1Dokument70 SeitenArianto Salim - Pemicu 1Mudita DewiNoch keine Bewertungen
- Jurnal ReadingDokument2 SeitenJurnal ReadingMudita DewiNoch keine Bewertungen
- Pemicu 5 GIT Mudita DewiDokument56 SeitenPemicu 5 GIT Mudita DewiMudita DewiNoch keine Bewertungen
- SalbutamolDokument2 SeitenSalbutamolMudita DewiNoch keine Bewertungen
- P7 Emergency BlockDokument35 SeitenP7 Emergency BlockMudita DewiNoch keine Bewertungen
- Group 7-Plenary 1-GI 2015Dokument41 SeitenGroup 7-Plenary 1-GI 2015Mudita DewiNoch keine Bewertungen
- PBL 1 GITDokument36 SeitenPBL 1 GITMudita DewiNoch keine Bewertungen
- Pemicu 1 KGD - DarrenDokument198 SeitenPemicu 1 KGD - DarrenMudita DewiNoch keine Bewertungen
- Pemicu 1 KGD - DarrenDokument198 SeitenPemicu 1 KGD - DarrenMudita DewiNoch keine Bewertungen
- Pemicu 2: Mudita Dewi 405150016Dokument43 SeitenPemicu 2: Mudita Dewi 405150016Mudita DewiNoch keine Bewertungen
- Pemicu 5 GITDokument52 SeitenPemicu 5 GITMudita DewiNoch keine Bewertungen
- Problem 1 GITDokument177 SeitenProblem 1 GITMudita DewiNoch keine Bewertungen
- Group 7-Plenary 1-GI 2015Dokument41 SeitenGroup 7-Plenary 1-GI 2015Mudita DewiNoch keine Bewertungen
- Pemicu 2 GIDokument123 SeitenPemicu 2 GIDessy DsyNoch keine Bewertungen
- Pemicu 1 Blok GiDokument35 SeitenPemicu 1 Blok GiMudita DewiNoch keine Bewertungen
- Pemicu 3 GITDokument143 SeitenPemicu 3 GITMudita DewiNoch keine Bewertungen
- PBL 1 GITDokument36 SeitenPBL 1 GITMudita DewiNoch keine Bewertungen
- Giraffe Blood CirculationDokument9 SeitenGiraffe Blood Circulationthalita asriandinaNoch keine Bewertungen
- Lbbbi18 Long Exam 1Dokument71 SeitenLbbbi18 Long Exam 1namkimseoNoch keine Bewertungen
- Complication of Blood TransfusionDokument5 SeitenComplication of Blood TransfusionChey Ochy ApriliaNoch keine Bewertungen
- Drugs Used in The Treatment of Congestive Heart FailureDokument18 SeitenDrugs Used in The Treatment of Congestive Heart Failurekarina azlia amandaNoch keine Bewertungen
- Steps of Repertorization - 5e097dab9ad98Dokument18 SeitenSteps of Repertorization - 5e097dab9ad98Sowjanya JyothsnaNoch keine Bewertungen
- Orthodontic Treatment in Systemic DisordersDokument9 SeitenOrthodontic Treatment in Systemic DisordersElizabeth Diaz BuenoNoch keine Bewertungen
- Extrapyramidal Side EffectsDokument15 SeitenExtrapyramidal Side EffectsNikhil YadavNoch keine Bewertungen
- Daftar Isi FormulariumDokument9 SeitenDaftar Isi FormulariumNilam atika sariNoch keine Bewertungen
- 342 FullDokument26 Seiten342 FullputrianabrsitompulNoch keine Bewertungen
- Cure Gum Disease Naturally Heal and Prevent AmazonindsjzoDokument6 SeitenCure Gum Disease Naturally Heal and Prevent Amazonindsjzocafechild05Noch keine Bewertungen
- Cellulitis Talk Jan 2018Dokument16 SeitenCellulitis Talk Jan 2018Ramsyifa VirzanisdaNoch keine Bewertungen
- Optometry - CounsellingDokument21 SeitenOptometry - CounsellingDashMadNoch keine Bewertungen
- Cholinergic System Model Questions & AnswersDokument45 SeitenCholinergic System Model Questions & AnswersDr.U.P.Rathnakar.MD.DIH.PGDHM100% (5)
- PHAR 400 Pharmacology I Master 1-3-21Dokument5 SeitenPHAR 400 Pharmacology I Master 1-3-21Zahid Bashir BhattiNoch keine Bewertungen
- Prevalence of Rifampicin Resistance Tuberculosis and Associated Factors Among Presumptive TB or MDRDokument3 SeitenPrevalence of Rifampicin Resistance Tuberculosis and Associated Factors Among Presumptive TB or MDRTigray OutlookNoch keine Bewertungen
- Brosur Katalog Medtek 2021Dokument12 SeitenBrosur Katalog Medtek 2021Dano CuyNoch keine Bewertungen
- NIV - Past, Present and FutureDokument9 SeitenNIV - Past, Present and FutureDejan ŽujovićNoch keine Bewertungen
- 12 Drugs Acting On The Cardiovascular SystemDokument5 Seiten12 Drugs Acting On The Cardiovascular SystemJAN CAMILLE LENONNoch keine Bewertungen
- Efficacy and Safety of Twice Vs Once Daily ALAADokument11 SeitenEfficacy and Safety of Twice Vs Once Daily ALAAOmar AyashNoch keine Bewertungen
- Jurnal Forensik Trauma KimiaDokument5 SeitenJurnal Forensik Trauma Kimiaikram hanafiNoch keine Bewertungen
- Computational Fluid Dynamics and Trigeminal Sensory Examinations of Empty Nose Syndrome PatientsDokument60 SeitenComputational Fluid Dynamics and Trigeminal Sensory Examinations of Empty Nose Syndrome Patientsmadhumitha srinivasNoch keine Bewertungen
- PricelistDokument71 SeitenPricelistBugar Wahyu PNoch keine Bewertungen