Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- Buku Ajar Ilmu Penyakit Dalam Universitas Airlangga PDFDokument351 SeitenBuku Ajar Ilmu Penyakit Dalam Universitas Airlangga PDFMyrna Evanda Adeline71% (7)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Outline For Teen DepressionDokument2 SeitenOutline For Teen Depressionapi-31726223650% (2)
- Volume 1 Blood, Iron and SulfurDokument18 SeitenVolume 1 Blood, Iron and Sulfursanjosewhore80% (20)
- E203 FullDokument2 SeitenE203 FullengkiiiNoch keine Bewertungen
- K5 - Disorders of Autonomic Nervous SystemDokument47 SeitenK5 - Disorders of Autonomic Nervous Systemengkiii100% (1)
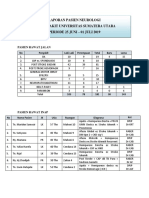
- Laporan Pasien Rs 25 Juni - 01 Juli 2019Dokument2 SeitenLaporan Pasien Rs 25 Juni - 01 Juli 2019engkiiiNoch keine Bewertungen
- Travellers and TraveloguesDokument11 SeitenTravellers and TraveloguesAlejandro FernoNoch keine Bewertungen
- Principles of TB Care and Prevention - Course Brief 2022Dokument2 SeitenPrinciples of TB Care and Prevention - Course Brief 2022Sherry CHENNoch keine Bewertungen
- Angelica M. Revil Docx CHN LFD No 2Dokument3 SeitenAngelica M. Revil Docx CHN LFD No 2Angelica Malacay RevilNoch keine Bewertungen
- Future Secure Private Car Package Policy Add On WordingsDokument25 SeitenFuture Secure Private Car Package Policy Add On WordingsRajeev Kumar PandeyNoch keine Bewertungen
- FILE 20220810 200849 Ta-Rv-12Dokument13 SeitenFILE 20220810 200849 Ta-Rv-12Hà ĐinhNoch keine Bewertungen
- LEV Medicine - Rejuvenation Research Guest EditorialDokument2 SeitenLEV Medicine - Rejuvenation Research Guest EditorialoliverNoch keine Bewertungen
- Student ServicesDokument19 SeitenStudent Servicesapi-297925543Noch keine Bewertungen
- Family Health Optima Insurance Plan NewDokument8 SeitenFamily Health Optima Insurance Plan NewNeeraj NemaNoch keine Bewertungen
- Mapeh 10 1st Periodical TestDokument4 SeitenMapeh 10 1st Periodical TestJunafel Boiser Garcia100% (3)
- WHO Road Safety 2023Dokument96 SeitenWHO Road Safety 2023govardhanrohanNoch keine Bewertungen
- Factors Affecting Health Care DemandDokument5 SeitenFactors Affecting Health Care DemandRochelle Anne Abad BandaNoch keine Bewertungen
- Excessive Occupational Heat Exposure: A Significant Ergonomic Challenge and Health Risk For Current and Future WorkersDokument9 SeitenExcessive Occupational Heat Exposure: A Significant Ergonomic Challenge and Health Risk For Current and Future WorkersEdna Odette Melo UscangaNoch keine Bewertungen
- Medical Health Examination FormDokument4 SeitenMedical Health Examination FormAldwin Bagtas0% (1)
- Matthew PerryDokument3 SeitenMatthew PerrydiogogamitoNoch keine Bewertungen
- CWPT Color Words Pick Out Test Available For Classifying The Slight Disorder On The Preclinical Stage of DementiaDokument5 SeitenCWPT Color Words Pick Out Test Available For Classifying The Slight Disorder On The Preclinical Stage of DementiaHerald Scholarly Open AccessNoch keine Bewertungen
- Vacation & LeaveDokument8 SeitenVacation & LeaveNephrology On-DemandNoch keine Bewertungen
- PC Bahasa Inggris UPK 22.Dokument16 SeitenPC Bahasa Inggris UPK 22.Blackes HoleNoch keine Bewertungen
- Literature Review Tabitha Satkamp 2Dokument4 SeitenLiterature Review Tabitha Satkamp 2api-608392349Noch keine Bewertungen
- NCM 120 Week 6 Topic 5Dokument83 SeitenNCM 120 Week 6 Topic 5Ma. Esperanza C. Eijansantos-Reavon50% (2)
- Measles Outbreak Response PlanDokument24 SeitenMeasles Outbreak Response PlanveroniqueNoch keine Bewertungen
- NursingDokument20 SeitenNursingCrazy StrangerNoch keine Bewertungen
- PSM 2020-2008 Regular Question Papers WBUHS © Medical JunctionDokument15 SeitenPSM 2020-2008 Regular Question Papers WBUHS © Medical JunctionJyotirmayeeNoch keine Bewertungen
- Complementary and Alternative Medicines Among ResiDokument10 SeitenComplementary and Alternative Medicines Among ResiKaye Reyes-HapinNoch keine Bewertungen
- Retelling The Good Samaritan PDFDokument6 SeitenRetelling The Good Samaritan PDFNicu CretuNoch keine Bewertungen
- Exploring The Effects of Social Media Use On The Mental Health ofDokument60 SeitenExploring The Effects of Social Media Use On The Mental Health ofapi-514461952Noch keine Bewertungen
- Vedic Astrology SaturnDokument131 SeitenVedic Astrology Saturnanannd100% (13)
- Essay On Mental Health AwarenessDokument2 SeitenEssay On Mental Health AwarenessHANNAH MADRONANoch keine Bewertungen
- Full Medical Examination Form For Foreign Workers: Work Pass DivisionDokument1 SeiteFull Medical Examination Form For Foreign Workers: Work Pass Divisionkarthik.swamyNoch keine Bewertungen