Das könnte Ihnen auch gefallen
- Case Report: Supevisor: Dr. Irma Tarida Listiawati, SP - KK By: Alif Ramadhan, S.KedDokument22 SeitenCase Report: Supevisor: Dr. Irma Tarida Listiawati, SP - KK By: Alif Ramadhan, S.Kedpang_paangNoch keine Bewertungen
- Leprosy (Morbus Hansen) : Dr. Uun Khusnul Khotimah, SPKKDokument38 SeitenLeprosy (Morbus Hansen) : Dr. Uun Khusnul Khotimah, SPKKagilNoch keine Bewertungen
- Leprosy: Hansen'S DiseaseDokument47 SeitenLeprosy: Hansen'S DiseaseTheo Grazila RuvaNoch keine Bewertungen
- Case 4. Leprosy and Reaction For Tutor Guide-Revisi 161120Dokument25 SeitenCase 4. Leprosy and Reaction For Tutor Guide-Revisi 161120Raihan IsvandiarNoch keine Bewertungen
- LeprosyDokument10 SeitenLeprosyRizweta DestinNoch keine Bewertungen
- Complete Dermatology NotesDokument41 SeitenComplete Dermatology NotesSetlhare MotsamaiNoch keine Bewertungen
- Case ReportDokument31 SeitenCase Reportchuck55Noch keine Bewertungen
- Tinea KorporisDokument25 SeitenTinea KorporisyustinanadaNoch keine Bewertungen
- Kemoterapi Lepra: Bag. Farmakologi Dan Terapi FK Undip 2017Dokument24 SeitenKemoterapi Lepra: Bag. Farmakologi Dan Terapi FK Undip 2017Yeni HerawatiNoch keine Bewertungen
- Lepra 2018Dokument56 SeitenLepra 2018abelNoch keine Bewertungen
- 30-3 Rrecurring Oral UlcerDokument31 Seiten30-3 Rrecurring Oral UlcerMax FaxNoch keine Bewertungen
- Dermatomyositis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsVon EverandDermatomyositis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNoch keine Bewertungen
- Leprosy SlideDokument23 SeitenLeprosy Slideandhika_938011069Noch keine Bewertungen
- How To Evaluate A Case of LeprosyDokument35 SeitenHow To Evaluate A Case of LeprosyBarath Kumar SinghNoch keine Bewertungen
- RetinoblastomaDokument24 SeitenRetinoblastomaMiguel Carlos Navarro Tacderan100% (1)
- Leprosy 22Dokument49 SeitenLeprosy 22Phc ChathannoorNoch keine Bewertungen
- DermatologyDokument259 SeitenDermatologyElma McGouganNoch keine Bewertungen
- LEPROSYDokument100 SeitenLEPROSYPratzNoch keine Bewertungen
- Pityriasis Alba-Common Disease, EnigmaticDokument21 SeitenPityriasis Alba-Common Disease, EnigmaticSartini Roma Dame NainggolanNoch keine Bewertungen
- L15 - Effect of Radiation 2Dokument41 SeitenL15 - Effect of Radiation 2Obahakam_917038774Noch keine Bewertungen
- Hansens Disease Presentation 3Dokument40 SeitenHansens Disease Presentation 3Princewill SmithNoch keine Bewertungen
- Dr. R. Sekhon - Dermatology Telehealth Jan 27 MRDokument45 SeitenDr. R. Sekhon - Dermatology Telehealth Jan 27 MRAnissa ADNoch keine Bewertungen
- HansensDokument83 SeitenHansensHrishikesh NachinolkarNoch keine Bewertungen
- M. LepraeDokument22 SeitenM. LepraeRina AlimuddinNoch keine Bewertungen
- Morbus HansenDokument48 SeitenMorbus HansenAyunda Henna PelalawanNoch keine Bewertungen
- Oleh: Dr. Septian Tri Muhari Pembimbing: Dr. Afifa Ramadanti, Sp.A (K)Dokument52 SeitenOleh: Dr. Septian Tri Muhari Pembimbing: Dr. Afifa Ramadanti, Sp.A (K)Septian TheaNoch keine Bewertungen
- Erythema Multiforme Major: Case Report and Review of LiteratureDokument6 SeitenErythema Multiforme Major: Case Report and Review of LiteratureSasa AprilaNoch keine Bewertungen
- Morbus HansenDokument37 SeitenMorbus HansenYolanda Agnesia Purba100% (1)
- Age Spots (Lentigines), A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsVon EverandAge Spots (Lentigines), A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNoch keine Bewertungen
- ONCOLOGYDokument29 SeitenONCOLOGYmendozaayajulienneNoch keine Bewertungen
- Section Slides 2Dokument52 SeitenSection Slides 2drsafwatismailNoch keine Bewertungen
- Dermotologic - BoardsDokument10 SeitenDermotologic - BoardsSoojung NamNoch keine Bewertungen
- Case PresentationDokument35 SeitenCase Presentationapi-498720485Noch keine Bewertungen
- Diagnosis and Recent Therapy of Fixed Drug EruptionDokument14 SeitenDiagnosis and Recent Therapy of Fixed Drug EruptionSheilaNoch keine Bewertungen
- LeprosyDokument51 SeitenLeprosySoujanya Kundu ChoudhuryNoch keine Bewertungen
- Kusta: Dr. M. Syafei Hamzah, SPKKDokument17 SeitenKusta: Dr. M. Syafei Hamzah, SPKKSarachanda SallyNoch keine Bewertungen
- Eritropapuloskuamosa Kuliah NewDokument52 SeitenEritropapuloskuamosa Kuliah NewpipitNoch keine Bewertungen
- Refarat Pytriasis VesicolorDokument18 SeitenRefarat Pytriasis VesicolormuselvindaNoch keine Bewertungen
- The Wound CareDokument51 SeitenThe Wound CareIosefina DudeanuNoch keine Bewertungen
- Morphea (Localized Scleroderma) : Is An Autoimmune Disease That Causes Sclerosis, or Scarlike, Changes To The SkinDokument1 SeiteMorphea (Localized Scleroderma) : Is An Autoimmune Disease That Causes Sclerosis, or Scarlike, Changes To The SkinMahmud AnshoriNoch keine Bewertungen
- Atmaja Sirupang-Journal Reading MHDokument9 SeitenAtmaja Sirupang-Journal Reading MHAtmaja R. SirupangNoch keine Bewertungen
- Prezentare TEN EnglezaDokument27 SeitenPrezentare TEN EnglezaAlinaNoch keine Bewertungen
- Erisipelas, Morbus Hansen, Dan DKA: Kelompok 7ADokument47 SeitenErisipelas, Morbus Hansen, Dan DKA: Kelompok 7Aelisabetheb kapaiterbakujayNoch keine Bewertungen
- Wound Dressing GuideDokument2 SeitenWound Dressing Guidekitsil100% (8)
- Hansens DiseaseDokument83 SeitenHansens DiseaseSajin AlexanderNoch keine Bewertungen
- MPDS & Developmental Disorder of TMJ - 20240210 - 123200 - 0000Dokument21 SeitenMPDS & Developmental Disorder of TMJ - 20240210 - 123200 - 0000NIVEDHA VAITHYANATHAN vNoch keine Bewertungen
- A Summary of LeprosyDokument80 SeitenA Summary of LeprosyJohnNoch keine Bewertungen
- Leprosy PowerpointDokument74 SeitenLeprosy PowerpointGeorgie May Almacen100% (1)
- Race Dermatology 2024 by DR AshishDokument29 SeitenRace Dermatology 2024 by DR AshishdrshekarforyouNoch keine Bewertungen
- Fibroma: Dr. Ishita Singhal Mds First YearDokument33 SeitenFibroma: Dr. Ishita Singhal Mds First YearDR. ISHITA SINGHALNoch keine Bewertungen
- Toxic Epidermal Necrolysis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsVon EverandToxic Epidermal Necrolysis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNoch keine Bewertungen
- Diagnosis and Treatment of Leprosy2Dokument27 SeitenDiagnosis and Treatment of Leprosy2abhishek chaudharyNoch keine Bewertungen
- SCROFULODERMADokument25 SeitenSCROFULODERMAFaradiba MaricarNoch keine Bewertungen
- Radiofrequencia MicroagulhamentoDokument7 SeitenRadiofrequencia MicroagulhamentoCristiane RalloNoch keine Bewertungen
- Pediatric DermatosesDokument58 SeitenPediatric DermatosesSajin AlexanderNoch keine Bewertungen
- Lesson Plan On Wound Care - With CommentsDokument7 SeitenLesson Plan On Wound Care - With CommentsJoyJoy Tabada CalunsagNoch keine Bewertungen
- Leprosy - One of The Few Diseases Which Can Be EliminatedDokument40 SeitenLeprosy - One of The Few Diseases Which Can Be EliminatedGendut GembrotNoch keine Bewertungen
- Headache, SkinDokument4 SeitenHeadache, SkinNadia SalwaniNoch keine Bewertungen
- Leprosy (1) - 230823 - 222046Dokument61 SeitenLeprosy (1) - 230823 - 222046Mushfiq RahmanNoch keine Bewertungen
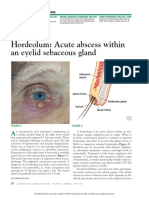
- Hordeolum: Acute Abscess Within An Eyelid Sebaceous Gland: The Clinical PictureDokument3 SeitenHordeolum: Acute Abscess Within An Eyelid Sebaceous Gland: The Clinical PictureCamNoch keine Bewertungen
- Urea Breath TestDokument92 SeitenUrea Breath TestBayan SNoch keine Bewertungen
- Muimar Sales PageDokument3 SeitenMuimar Sales PagePre Boy Ent.Noch keine Bewertungen
- JaundiceDokument42 SeitenJaundiceMaitry PatelNoch keine Bewertungen
- Homework: 1) What Does The Respiratory System Do ?Dokument6 SeitenHomework: 1) What Does The Respiratory System Do ?Mariana VasileNoch keine Bewertungen
- What Is EczemaDokument9 SeitenWhat Is EczemaChoo YieNoch keine Bewertungen
- Ophthalmology For The Equine Practitioner 2002-2002Dokument2 SeitenOphthalmology For The Equine Practitioner 2002-2002Francisco JulianNoch keine Bewertungen
- Communicable Disease NursingDokument41 SeitenCommunicable Disease NursingPagarigan VianNoch keine Bewertungen
- Bernardino Ramazzini (1633-1714)Dokument2 SeitenBernardino Ramazzini (1633-1714)uknandiNoch keine Bewertungen
- Daftar Singkatan DiagnosaDokument5 SeitenDaftar Singkatan DiagnosaNIRMALANoch keine Bewertungen
- English Communication in NurseDokument7 SeitenEnglish Communication in NurseSiti NuraisiahNoch keine Bewertungen
- Relapsing Polychondritis: Presented By: Fatima AhmedDokument19 SeitenRelapsing Polychondritis: Presented By: Fatima AhmedAamna HumayounNoch keine Bewertungen
- NCP Inflamed TonsillitisDokument3 SeitenNCP Inflamed TonsillitisAubrey LafuenteNoch keine Bewertungen
- Progyluton-26 1DDokument16 SeitenProgyluton-26 1DUsma aliNoch keine Bewertungen
- PlagueDokument20 SeitenPlagueHemanth G.Noch keine Bewertungen
- Annex A. Individual BMI Report: School Health ServicesDokument3 SeitenAnnex A. Individual BMI Report: School Health ServicesSusan Loida SorianoNoch keine Bewertungen
- 58 Iajps58122019 PDFDokument4 Seiten58 Iajps58122019 PDFiajpsNoch keine Bewertungen
- Pediatric ICD-10-CM Coding Tip Sheet: Overview of Key Chapter Updates For Pediatric and Top 25 CodesDokument4 SeitenPediatric ICD-10-CM Coding Tip Sheet: Overview of Key Chapter Updates For Pediatric and Top 25 CodesAmerican Aesthetic MCNoch keine Bewertungen
- Life Style DiseasesDokument19 SeitenLife Style DiseasesAnjana BabuNoch keine Bewertungen
- Journal CritiueDokument2 SeitenJournal CritiueJajangNoch keine Bewertungen
- What Is A Heart Transplant?Dokument2 SeitenWhat Is A Heart Transplant?Michael MirasolNoch keine Bewertungen
- Names (M) : Nutritional Status ReportDokument7 SeitenNames (M) : Nutritional Status ReportGrace V Mae JaymeNoch keine Bewertungen
- BACTERIAL DISEASES in Marine MammalsDokument15 SeitenBACTERIAL DISEASES in Marine MammalsAndre Val CamarintaNoch keine Bewertungen
- Wagenigen UniversityDokument45 SeitenWagenigen UniversityAyu Lidya NingsihNoch keine Bewertungen
- OsteoarthritisDokument29 SeitenOsteoarthritischan park100% (1)
- Guidelines For International Arrival 20 TH October 2021Dokument3 SeitenGuidelines For International Arrival 20 TH October 2021Republic WorldNoch keine Bewertungen
- Case Study Femoral Acetabular Impingement (FAI)Dokument21 SeitenCase Study Femoral Acetabular Impingement (FAI)Ah ZhangNoch keine Bewertungen
- Sample Doctors Note For StudentDokument1 SeiteSample Doctors Note For StudentWaldo SchobbenNoch keine Bewertungen
- Open RubricDokument71 SeitenOpen RubricNgcwalisa Ntwalana100% (1)
- 8 Human Health N Disease-NotesDokument5 Seiten8 Human Health N Disease-NotesAnanth DharanidharanNoch keine Bewertungen
- Excercise 2 - Frequency MeasureDokument6 SeitenExcercise 2 - Frequency MeasureAnonymous aH8gCZ7zj75% (4)