Das könnte Ihnen auch gefallen
- Head InjuryDokument50 SeitenHead InjuryThiagarajah RaviNoch keine Bewertungen
- HEAD INJURY (Trauma Kepala) DR - AgusDokument53 SeitenHEAD INJURY (Trauma Kepala) DR - AgusSetyo RahmanNoch keine Bewertungen
- Head Trauma: Initial Assessment and ManagementDokument38 SeitenHead Trauma: Initial Assessment and Managementi wayan dediyanaNoch keine Bewertungen
- Head Injury AnesDokument42 SeitenHead Injury Aneskenbon kenbonNoch keine Bewertungen
- Introduction To Neurosurgical Subspecialties Trauma and Critical Care NeurosurgeryDokument26 SeitenIntroduction To Neurosurgical Subspecialties Trauma and Critical Care NeurosurgeryMuhammad Azhary LazuardyNoch keine Bewertungen
- Brain TumorDokument43 SeitenBrain TumorjeremiahNoch keine Bewertungen
- Head Injury 5Dokument68 SeitenHead Injury 5drvishal bhattNoch keine Bewertungen
- Sunkara DB Neurological DisordersDokument41 SeitenSunkara DB Neurological DisordersAngela SaoNoch keine Bewertungen
- Head Trauma: Dr. Andy Wijaya, SpemDokument20 SeitenHead Trauma: Dr. Andy Wijaya, SpemThomas AlbertNoch keine Bewertungen
- Headache Neuroimaging FinalDokument85 SeitenHeadache Neuroimaging Finaldinesh kumarNoch keine Bewertungen
- CPP Monitoring for Cerebral Perfusion AssessmentDokument131 SeitenCPP Monitoring for Cerebral Perfusion AssessmentEMBER MARIE SAYMANNoch keine Bewertungen
- An Overview of Head Injury Management: Eldad J. Hadar, M.DDokument35 SeitenAn Overview of Head Injury Management: Eldad J. Hadar, M.DBirhanu ShiferawNoch keine Bewertungen
- Brain TraumaDokument32 SeitenBrain Traumafrengki kobogauNoch keine Bewertungen
- Head Injuries 2015Dokument41 SeitenHead Injuries 2015jimmyNoch keine Bewertungen
- head injuryDokument39 Seitenhead injuryYonathan asnakeNoch keine Bewertungen
- Traumatic Brain Injury (TBI) : Epidural Hematoma Subdural HematomaDokument62 SeitenTraumatic Brain Injury (TBI) : Epidural Hematoma Subdural HematomaRey AlwiwikhNoch keine Bewertungen
- NeurologyDokument37 SeitenNeurologyDevangkumar PatelNoch keine Bewertungen
- 01 Neurologic Conditions WDokument133 Seiten01 Neurologic Conditions WBenzy Anne MermalNoch keine Bewertungen
- CBT Neurosurgery - TutorDokument24 SeitenCBT Neurosurgery - Tutoramoody95Noch keine Bewertungen
- Untitled 5Dokument23 SeitenUntitled 5EBNoch keine Bewertungen
- Cedera KepalaDokument33 SeitenCedera Kepalahali100% (1)
- Head TraumaDokument32 SeitenHead Traumajeevan kumar reddyNoch keine Bewertungen
- Trauma - Head Injuries: S.Mohganasundram S1Dokument43 SeitenTrauma - Head Injuries: S.Mohganasundram S1Nazee NazreenNoch keine Bewertungen
- Head Injury EciDokument29 SeitenHead Injury EciYullytia Galaksi MharyatiNoch keine Bewertungen
- Neurologic Trauma: Traumatic Brain InjuryDokument18 SeitenNeurologic Trauma: Traumatic Brain InjuryPearl Raiza Hadani100% (1)
- Acute Surgical Management: Sharitadevi Christevan Daniswari 1710221029Dokument26 SeitenAcute Surgical Management: Sharitadevi Christevan Daniswari 1710221029daaaniiisNoch keine Bewertungen
- Brain InjuryDokument35 SeitenBrain InjuryAkhil Adhithyan RamNoch keine Bewertungen
- Head Injury GoulburnDokument47 SeitenHead Injury GoulburnSyarifah Maisyura100% (1)
- Head InjuryDokument36 SeitenHead InjuryNorFarah Fatin AnuarNoch keine Bewertungen
- Head Trauma: Types of Resulting Brain InjuryDokument6 SeitenHead Trauma: Types of Resulting Brain InjuryAnjali ParajuliNoch keine Bewertungen
- Head Trauma & Management: Dr. Utham Murali. M.S M.B.A. Asso - Prof of Surgery IMS / MSU / MalaysiaDokument48 SeitenHead Trauma & Management: Dr. Utham Murali. M.S M.B.A. Asso - Prof of Surgery IMS / MSU / MalaysiaNinaNoch keine Bewertungen
- Head Injury 2022.Dokument45 SeitenHead Injury 2022.Alia QNoch keine Bewertungen
- Kuliah Head Injury MakasarDokument113 SeitenKuliah Head Injury MakasarJerrod WilsonNoch keine Bewertungen
- Intra-Cranial Hemorrhage EDH SDH SAH Acute SDH Chronic SDHDokument8 SeitenIntra-Cranial Hemorrhage EDH SDH SAH Acute SDH Chronic SDHZuhra JabeenNoch keine Bewertungen
- 4th Problem Emergency Medicine Group 1Dokument82 Seiten4th Problem Emergency Medicine Group 1Jonathan TandajuNoch keine Bewertungen
- Head Injury 2Dokument47 SeitenHead Injury 2drvishal bhattNoch keine Bewertungen
- Traumatic Head InjuriesDokument50 SeitenTraumatic Head InjuriesVasudha BuddyNoch keine Bewertungen
- General Surgery Trauma (Head and Thorax)Dokument24 SeitenGeneral Surgery Trauma (Head and Thorax)Noora AlmuailiNoch keine Bewertungen
- Head InjuryDokument47 SeitenHead InjuryRio Taruna JatiNoch keine Bewertungen
- STROKE SYNDROMESDokument37 SeitenSTROKE SYNDROMESGROUP 1 2023Noch keine Bewertungen
- Management OF Head Injury: DR Echebiri, PDokument26 SeitenManagement OF Head Injury: DR Echebiri, PLuther ThengNoch keine Bewertungen
- Head Injury PediaDokument44 SeitenHead Injury PediaReena MittalNoch keine Bewertungen
- 9 - Management of Patients With Neurological TraumaDokument33 Seiten9 - Management of Patients With Neurological TraumaTaif SalimNoch keine Bewertungen
- An Overview of Head Injury Management: Eldad J. Hadar, M.DDokument35 SeitenAn Overview of Head Injury Management: Eldad J. Hadar, M.DIbnu Fadirul WahedNoch keine Bewertungen
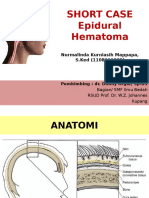
- SHORT CASE 1 Epidural HematomaDokument30 SeitenSHORT CASE 1 Epidural HematomaNurmalinda MappapaNoch keine Bewertungen
- Headache Management in Primary CareDokument59 SeitenHeadache Management in Primary Carechyntia eryonza100% (1)
- Head Trauma DR Petra SPBSDokument64 SeitenHead Trauma DR Petra SPBSAlessia Wyneini TirzaNoch keine Bewertungen
- Craniocerebral Injury/ Head InjuryDokument36 SeitenCraniocerebral Injury/ Head InjurySamjhana GautamNoch keine Bewertungen
- Dr. Tommy SP - BS - Head Trauma Webinar Dr. TMYDokument30 SeitenDr. Tommy SP - BS - Head Trauma Webinar Dr. TMYOctafiani Trikartika DarimanNoch keine Bewertungen
- Neurologic and Neurosurgical Emergencies For Nursing StudentsDokument39 SeitenNeurologic and Neurosurgical Emergencies For Nursing StudentsDr Ganeshgouda MajigoudraNoch keine Bewertungen
- HEAD INJURY Presentation HDDokument29 SeitenHEAD INJURY Presentation HDRed DevilNoch keine Bewertungen
- Cedera Kepala Dan Otak: Dr. Isnaniah, Sp. S Bagian Saraf Fkik UntadDokument91 SeitenCedera Kepala Dan Otak: Dr. Isnaniah, Sp. S Bagian Saraf Fkik UntadSiwa MerthadinataNoch keine Bewertungen
- Brain DeathDokument65 SeitenBrain DeathAnupam SarkarNoch keine Bewertungen
- CT Scans of The Head: A Neurologist's Perspective: Lara Cooke January 15, 2009Dokument111 SeitenCT Scans of The Head: A Neurologist's Perspective: Lara Cooke January 15, 2009adrian100% (1)
- Brain Hemorrhage and Dementia GuideDokument42 SeitenBrain Hemorrhage and Dementia Guidevenia endah tamaraNoch keine Bewertungen
- Chapter 2 Intro To Brain ImagingDokument49 SeitenChapter 2 Intro To Brain ImagingJellie MendozaNoch keine Bewertungen
- Head Injury by Dr. Keiza .NDokument32 SeitenHead Injury by Dr. Keiza .NIrene Zae MwandotoNoch keine Bewertungen
- Head Traumas: Anthony Safi Mediii Neurosurgery RotationDokument17 SeitenHead Traumas: Anthony Safi Mediii Neurosurgery RotationAnthony safiNoch keine Bewertungen
- Head Trauma: Dr. Nasir Lamhot, Sp. BSDokument31 SeitenHead Trauma: Dr. Nasir Lamhot, Sp. BSYohannes KurniawanNoch keine Bewertungen
- Disorders of Consciousness: Raymond Rheza 406138024Dokument8 SeitenDisorders of Consciousness: Raymond Rheza 406138024Elfa RiniNoch keine Bewertungen
- Remon CVD HemoragikDokument23 SeitenRemon CVD HemoragikElfa RiniNoch keine Bewertungen
- Os NasaleDokument4 SeitenOs NasaleElfa RiniNoch keine Bewertungen
- Sinusitis and Respiratory Disease at Pediatric AgeDokument5 SeitenSinusitis and Respiratory Disease at Pediatric AgeElfa RiniNoch keine Bewertungen
- Opening of blocked bank account and data sharing consentDokument1 SeiteOpening of blocked bank account and data sharing consentElfa RiniNoch keine Bewertungen
- ACLS ElfaDokument22 SeitenACLS ElfaElfa RiniNoch keine Bewertungen
- Aprovel-Slide RTD - The Importance of Microalbuminuria As A Target Therapy in Patients With Hypertension and CKD 2015-1Dokument42 SeitenAprovel-Slide RTD - The Importance of Microalbuminuria As A Target Therapy in Patients With Hypertension and CKD 2015-1Elfa RiniNoch keine Bewertungen
- Penanganan Sepsis PitDokument43 SeitenPenanganan Sepsis PitElfa RiniNoch keine Bewertungen
- Referat Terapi Hipertensi Restisten Elfarini 406151044Dokument19 SeitenReferat Terapi Hipertensi Restisten Elfarini 406151044Elfa RiniNoch keine Bewertungen
- A Study of Correlation Between Subjective Sensation of Nose Block and Objective Assessment of Nasal Patency by Cold Spatula Test in A Patient With Nose BlockDokument5 SeitenA Study of Correlation Between Subjective Sensation of Nose Block and Objective Assessment of Nasal Patency by Cold Spatula Test in A Patient With Nose BlockElfa RiniNoch keine Bewertungen
- Mitochondrial DNA Mutations Associated With AminoglycosideDokument8 SeitenMitochondrial DNA Mutations Associated With AminoglycosideElfa RiniNoch keine Bewertungen
- A Study of Correlation Between Subjective Sensation of Nose Block and Objective Assessment of Nasal Patency by Cold Spatula Test in A Patient With Nose BlockDokument5 SeitenA Study of Correlation Between Subjective Sensation of Nose Block and Objective Assessment of Nasal Patency by Cold Spatula Test in A Patient With Nose BlockElfa RiniNoch keine Bewertungen
- Referat Terapi Hipertensi Restisten ElfaDokument19 SeitenReferat Terapi Hipertensi Restisten ElfaElfa RiniNoch keine Bewertungen
- Istc TB AnakDokument68 SeitenIstc TB AnakElfa RiniNoch keine Bewertungen
- Ringkasan Tugas NeviDokument2 SeitenRingkasan Tugas NeviElfa RiniNoch keine Bewertungen
- Distosia Bahu Elfa BARUDokument24 SeitenDistosia Bahu Elfa BARUElfa RiniNoch keine Bewertungen
- NeviDokument3 SeitenNeviElfa RiniNoch keine Bewertungen
- Melanoma PictDokument3 SeitenMelanoma PictElfa RiniNoch keine Bewertungen
- Disorders of Consciousness: Raymond Rheza 406138024Dokument8 SeitenDisorders of Consciousness: Raymond Rheza 406138024Elfa RiniNoch keine Bewertungen
- Referat Distosia Bahu ElfaDokument16 SeitenReferat Distosia Bahu ElfaElfa RiniNoch keine Bewertungen
- 7 ImunisasiDokument85 Seiten7 ImunisasiElfa RiniNoch keine Bewertungen
- Distosia Bahu Elfa BARUDokument24 SeitenDistosia Bahu Elfa BARUElfa RiniNoch keine Bewertungen
- ACUTE ABDOMEN 02 O8-No.1Dokument77 SeitenACUTE ABDOMEN 02 O8-No.1Elfa RiniNoch keine Bewertungen
- Dietary Recall AnitaDokument6 SeitenDietary Recall AnitaElfa RiniNoch keine Bewertungen
- How to Treat Parkinson's DiseaseDokument18 SeitenHow to Treat Parkinson's DiseaseIpenPagarNoch keine Bewertungen
- Dizziness and VertigoDokument1 SeiteDizziness and VertigoElfa RiniNoch keine Bewertungen
- Reti No Blast OmaDokument10 SeitenReti No Blast OmaElfa RiniNoch keine Bewertungen
- Source For ReferatDokument1 SeiteSource For ReferatElfa RiniNoch keine Bewertungen
- Post Test-Module 5 H.O.P.E 12Dokument1 SeitePost Test-Module 5 H.O.P.E 12Kirby BrizNoch keine Bewertungen
- Republic of The Philippines Department of Education Region Iv-A Calabzon Division of Quezon Catanauan, QuezonDokument2 SeitenRepublic of The Philippines Department of Education Region Iv-A Calabzon Division of Quezon Catanauan, QuezonJayson Barsana100% (1)
- Bone FracturesDokument21 SeitenBone FracturesChintya Fidelia MontangNoch keine Bewertungen
- Classification of InjuriesDokument14 SeitenClassification of InjuriesAbhilash JanakkiNoch keine Bewertungen
- Endotracheal Tube ETT Insertion IntubationDokument3 SeitenEndotracheal Tube ETT Insertion IntubationmochkurniawanNoch keine Bewertungen
- 12 Physical Education Hindi Medium Chapter 9Dokument27 Seiten12 Physical Education Hindi Medium Chapter 9KRISHAN KUMAR100% (1)
- BLS ButuanDokument4 SeitenBLS ButuanHarbyNoch keine Bewertungen
- Musculoskeletal Injuries GuideDokument38 SeitenMusculoskeletal Injuries GuideWindi PradnyanaNoch keine Bewertungen
- Outcomes of Selective Non-Operative Management for Penetrating Splenic InjuryDokument44 SeitenOutcomes of Selective Non-Operative Management for Penetrating Splenic Injuryমোহাম্মদ আবীর100% (1)
- Pengkajian Luka Bates JensenDokument6 SeitenPengkajian Luka Bates JensenocsitaocsitulNoch keine Bewertungen
- Fractures of The Upper Limb: Dr. Salman AbbasiDokument60 SeitenFractures of The Upper Limb: Dr. Salman AbbasiSeimal MahmoodNoch keine Bewertungen
- Mechanical Injuries - LacerationsDokument55 SeitenMechanical Injuries - LacerationsFatema AminNoch keine Bewertungen
- Shoulder DislocationDokument17 SeitenShoulder DislocationFlavia KennadyNoch keine Bewertungen
- Ankle Fractures ExplainedDokument2 SeitenAnkle Fractures ExplainedSidney SaweNoch keine Bewertungen
- Advanced Cardiac Life Support (ACLS) : Dr. Martha Regisna Silalahi RSUD BintanDokument19 SeitenAdvanced Cardiac Life Support (ACLS) : Dr. Martha Regisna Silalahi RSUD BintangisnamarthaNoch keine Bewertungen
- Musculoskeletal TraumaDokument63 SeitenMusculoskeletal Traumarobby pardiansyahNoch keine Bewertungen
- Lesson 1 Safety Practices in Sports and ExerciseDokument17 SeitenLesson 1 Safety Practices in Sports and ExerciseMr. CRAFTNoch keine Bewertungen
- Tatalaksana Awal Cedera KepalaDokument24 SeitenTatalaksana Awal Cedera KepalaRamadhan HumaidiNoch keine Bewertungen
- Chapter 3 - WoundDokument37 SeitenChapter 3 - Woundwp6mq5bb25Noch keine Bewertungen
- Susi Erawati-Fkik PDFDokument116 SeitenSusi Erawati-Fkik PDFCholifaturrizkiyahNoch keine Bewertungen
- First Aid PPT Final DemonstratiomDokument24 SeitenFirst Aid PPT Final DemonstratiomRolly75% (4)
- Emergency Management of Subdural Hematoma: Corresponding Author: Abdulrahman Mubarak Almutairi - 0564804048Dokument3 SeitenEmergency Management of Subdural Hematoma: Corresponding Author: Abdulrahman Mubarak Almutairi - 0564804048Falon PapalangiNoch keine Bewertungen
- Head Trauma - Dr. Affan Priyambodo, SPBS (K)Dokument32 SeitenHead Trauma - Dr. Affan Priyambodo, SPBS (K)Verty SalleNoch keine Bewertungen
- Exceed Course Outline Osmak Post Grad Course PDFDokument6 SeitenExceed Course Outline Osmak Post Grad Course PDFAivoree SisonNoch keine Bewertungen
- EMS Protocols GuideDokument326 SeitenEMS Protocols GuideRaluca LupuNoch keine Bewertungen
- Cardiopulmonary Resuscitation (CPR) : First AidDokument5 SeitenCardiopulmonary Resuscitation (CPR) : First AidJules RyanNoch keine Bewertungen
- Sport InjuryDokument8 SeitenSport InjuryMohd MujahidNoch keine Bewertungen
- Case Presentation on a 50-Year-Old Male with Pelvic TraumaDokument15 SeitenCase Presentation on a 50-Year-Old Male with Pelvic TraumaAyesha JadoonNoch keine Bewertungen
- Nursing Wound AssessmentDokument3 SeitenNursing Wound AssessmentMatthew RyanNoch keine Bewertungen
- Safety Practices and Sports Injury Management.Dokument8 SeitenSafety Practices and Sports Injury Management.cejaygecainNoch keine Bewertungen