Das könnte Ihnen auch gefallen
- Hirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsVon EverandHirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNoch keine Bewertungen
- Care of Unconscious PatientDokument7 SeitenCare of Unconscious PatientSallieNoch keine Bewertungen
- Management of Tuberculosis: A guide for clinicians (eBook edition)Von EverandManagement of Tuberculosis: A guide for clinicians (eBook edition)Noch keine Bewertungen
- Lesson Plan BMA&BDokument14 SeitenLesson Plan BMA&BLoma Waghmare (Jadhav)Noch keine Bewertungen
- Hemodynamic MonitoringDokument4 SeitenHemodynamic Monitoringgurneet kourNoch keine Bewertungen
- Teaching Module Hypertension PregnancyDokument17 SeitenTeaching Module Hypertension PregnancyQueenie BlasurcaNoch keine Bewertungen
- SEIZURE DISORDER: CAUSES, TYPES, SIGNS AND TREATMENTDokument70 SeitenSEIZURE DISORDER: CAUSES, TYPES, SIGNS AND TREATMENTRohini RaiNoch keine Bewertungen
- Colostomy CareDokument2 SeitenColostomy CareMel RodolfoNoch keine Bewertungen
- Venturi face mask oxygen therapy procedureDokument2 SeitenVenturi face mask oxygen therapy procedureRosintchi MirsalNoch keine Bewertungen
- Myelography Procedure and Indications ExplainedDokument12 SeitenMyelography Procedure and Indications ExplainedDiana CharaNoch keine Bewertungen
- Assessing Newborns EffectivelyDokument35 SeitenAssessing Newborns EffectivelyBaldwin Hamzcorp Hamoonga100% (1)
- A Study To Assess The Effectiveness of Foot Massage On The Level of Pain Among Post-Operative Patients at Dhanush Hospital BagalkotDokument7 SeitenA Study To Assess The Effectiveness of Foot Massage On The Level of Pain Among Post-Operative Patients at Dhanush Hospital BagalkotInternational Journal of Innovative Science and Research TechnologyNoch keine Bewertungen
- Health Problems MyselfDokument54 SeitenHealth Problems MyselfKrishnaveni Murugesh100% (2)
- 5B Assessing Apical Pulse-2Dokument4 Seiten5B Assessing Apical Pulse-2Marky RoqueNoch keine Bewertungen
- Pulmonary ContusionDokument83 SeitenPulmonary ContusionLouise Anne Agnazata GayoNoch keine Bewertungen
- Types of Skin Traction PresentationDokument16 SeitenTypes of Skin Traction PresentationZerjohn Seniorom100% (1)
- Arterial Blood Gas ABG: Study GuideDokument6 SeitenArterial Blood Gas ABG: Study GuideDan Dan ManaoisNoch keine Bewertungen
- Measuring Body TemperatureDokument5 SeitenMeasuring Body TemperatureJan Jamison ZuluetaNoch keine Bewertungen
- Oesophageal Atresia by GabriellaDokument7 SeitenOesophageal Atresia by GabriellaGabrielleNoch keine Bewertungen
- Nso AbdurasadDokument4 SeitenNso AbdurasadNader AbdurasadNoch keine Bewertungen
- NephritisDokument21 SeitenNephritisruchikaNoch keine Bewertungen
- OSCE Subcutaneous Injection SkillsDokument2 SeitenOSCE Subcutaneous Injection SkillsvishnuNoch keine Bewertungen
- Physical Examination 2003Dokument39 SeitenPhysical Examination 2003Gayatri MudliyarNoch keine Bewertungen
- Nasal Instillation Procedure Guide NursingDokument2 SeitenNasal Instillation Procedure Guide NursingTrisha ApillanesNoch keine Bewertungen
- Health PromotionDokument34 SeitenHealth PromotionseljaNoch keine Bewertungen
- Tracheostomy CareDokument1 SeiteTracheostomy CareShreyas WalvekarNoch keine Bewertungen
- Sub - Medical Surgical Nursing: Assignment On CVP MonitoringDokument11 SeitenSub - Medical Surgical Nursing: Assignment On CVP Monitoringkamini ChoudharyNoch keine Bewertungen
- Oropharyngeal Airway InsertionDokument6 SeitenOropharyngeal Airway InsertionydtrgnNoch keine Bewertungen
- Endotracheal IntubationDokument5 SeitenEndotracheal Intubationpriyanka bhavsarNoch keine Bewertungen
- ETT IntubationDokument10 SeitenETT IntubationPoova RagavanNoch keine Bewertungen
- Airway SuctioningDokument30 SeitenAirway SuctioningPearl DiBerardinoNoch keine Bewertungen
- OxygenationDokument50 SeitenOxygenationLulu MushiNoch keine Bewertungen
- Fundal Height MeasurementDokument4 SeitenFundal Height MeasurementChanta MaharjanNoch keine Bewertungen
- CP On AGEDokument31 SeitenCP On AGELeah CaressaNoch keine Bewertungen
- BSN Year I Lesson Plan on MalariaDokument2 SeitenBSN Year I Lesson Plan on MalariaNaqash HamayunNoch keine Bewertungen
- Trends & Issues in MSN NursingDokument41 SeitenTrends & Issues in MSN NursingRajesh Sharma100% (3)
- NG Tube, Lavage and Gavage Procedure ChecklistDokument6 SeitenNG Tube, Lavage and Gavage Procedure ChecklistBitew Tefera ZewudieNoch keine Bewertungen
- Assisting With Arterial Puncture For Blood Gas Analysis EquipmentDokument7 SeitenAssisting With Arterial Puncture For Blood Gas Analysis EquipmentPoova RagavanNoch keine Bewertungen
- 12th Botany Sura Guide New Edition 2021-2022 English Medium Download PDF - WWW - Kalvikadal.inDokument43 Seiten12th Botany Sura Guide New Edition 2021-2022 English Medium Download PDF - WWW - Kalvikadal.inshariqueabdulazeez40Noch keine Bewertungen
- Chest Tube InsertionDokument4 SeitenChest Tube Insertionreiche100% (1)
- Respiratory Distress SyndromeDokument41 SeitenRespiratory Distress Syndromef.abrahamNoch keine Bewertungen
- Assisting Lumbar Puncture: By: Bonifacio P. Marilao Jr. Kirstine Anne Camille F. NuezDokument25 SeitenAssisting Lumbar Puncture: By: Bonifacio P. Marilao Jr. Kirstine Anne Camille F. NuezTheSweetpea501Noch keine Bewertungen
- Urine Albumin Test Detects Pregnancy RiskDokument7 SeitenUrine Albumin Test Detects Pregnancy RiskKaren Jae Grant CabrillosNoch keine Bewertungen
- Vital SignDokument4 SeitenVital SignGabriel JocsonNoch keine Bewertungen
- Education Sub Cutaneous Injection Lesson PlanDokument12 SeitenEducation Sub Cutaneous Injection Lesson Planamrutha h s100% (1)
- Script For EcgDokument14 SeitenScript For EcgMonesa Badil LingasaNoch keine Bewertungen
- Tracheostomy CareDokument41 SeitenTracheostomy CareBautista Aubergine100% (2)
- CVP MonitoringDokument24 SeitenCVP MonitoringChoji Heiwajima100% (1)
- AttachmentDokument26 SeitenAttachmentEliza AmandoNoch keine Bewertungen
- Administration of Inotropes Evidence Based Nursing PolicyDokument8 SeitenAdministration of Inotropes Evidence Based Nursing PolicyRonald ThakorNoch keine Bewertungen
- Nephro Case StudyDokument26 SeitenNephro Case Studyanimesh pandaNoch keine Bewertungen
- Topical skin procedure checklistDokument5 SeitenTopical skin procedure checklistpramod kumawatNoch keine Bewertungen
- Renal CalculiDokument11 SeitenRenal CalculiAaqashh MasseyNoch keine Bewertungen
- CATHETERIZATION ChecklistDokument2 SeitenCATHETERIZATION Checklistjmmos207064Noch keine Bewertungen
- Seminar On ETDokument10 SeitenSeminar On ETISLAMIC KNOWLEDGE BASED ON TRULY HADISNoch keine Bewertungen
- Tepid Sponge/Cold SpongeDokument2 SeitenTepid Sponge/Cold SpongeCheryl PorpayasNoch keine Bewertungen
- Treatment Aspects in Perioperative NursingDokument51 SeitenTreatment Aspects in Perioperative NursingShibin Jacob100% (2)
- COPDDokument15 SeitenCOPDUmapreethi Kumar100% (1)
- Partograph BoDokument60 SeitenPartograph BoRendy Adhitya PratamaNoch keine Bewertungen
- Partograph: A Graphical Record Of Labor Progress And ConditionsDokument49 SeitenPartograph: A Graphical Record Of Labor Progress And Conditionsdr jai gurungNoch keine Bewertungen
- Student Nurse Eye Assessment Emergency RoomDokument2 SeitenStudent Nurse Eye Assessment Emergency Roomharley dela cruzNoch keine Bewertungen
- 2019 PuerperumDokument15 Seiten2019 Puerperumharley dela cruzNoch keine Bewertungen
- DeathByAgeGroup PDFDokument3 SeitenDeathByAgeGroup PDFMarlon Vincent CabatoNoch keine Bewertungen
- DeathByAgeGroup PDFDokument3 SeitenDeathByAgeGroup PDFMarlon Vincent CabatoNoch keine Bewertungen
- DocumentationandreportingDokument43 SeitenDocumentationandreportingharley dela cruzNoch keine Bewertungen
- 2019 5framework of Health AssessmentDokument31 Seiten2019 5framework of Health Assessmentharley dela cruzNoch keine Bewertungen
- DocumentationandreportingDokument43 SeitenDocumentationandreportingharley dela cruzNoch keine Bewertungen
- DeathByAgeGroup PDFDokument3 SeitenDeathByAgeGroup PDFMarlon Vincent CabatoNoch keine Bewertungen
- Documentationand Nursing InformaticsDokument36 SeitenDocumentationand Nursing Informaticsharley dela cruzNoch keine Bewertungen
- WHO PartographDokument59 SeitenWHO PartographAnonymous 0C4OZmR100% (3)
- 2019 PARTPGRAPH DOH Maternalneonatal - CompressedDokument84 Seiten2019 PARTPGRAPH DOH Maternalneonatal - Compressedharley dela cruz100% (1)
- 2019 Intake and Output MeasurementDokument2 Seiten2019 Intake and Output Measurementharley dela cruzNoch keine Bewertungen
- 2018 PLQ - Chapter004Dokument2 Seiten2018 PLQ - Chapter004harley dela cruzNoch keine Bewertungen
- DocumentationandreportingDokument43 SeitenDocumentationandreportingharley dela cruzNoch keine Bewertungen
- Pre-Lecture Quiz Chapter 5 Critical ThinkingDokument2 SeitenPre-Lecture Quiz Chapter 5 Critical Thinkingharley dela cruzNoch keine Bewertungen
- 2018 PLQ - Chapter006Dokument2 Seiten2018 PLQ - Chapter006harley dela cruzNoch keine Bewertungen
- Common Medical Abbreviations and Lingo Seen in Nuc Med: A List of Useful Shorthand For History Taking and Chart ReviewingDokument6 SeitenCommon Medical Abbreviations and Lingo Seen in Nuc Med: A List of Useful Shorthand For History Taking and Chart Reviewingharley dela cruzNoch keine Bewertungen
- Tugas Dialog EnglishDokument4 SeitenTugas Dialog EnglishnuritaNoch keine Bewertungen
- MisoprostolDokument60 SeitenMisoprostolRaymonde UyNoch keine Bewertungen
- Antenatal Assessment of Fetal Well Being: DR - Abdulkarim Ahmed MohamudDokument46 SeitenAntenatal Assessment of Fetal Well Being: DR - Abdulkarim Ahmed MohamudPeterNoch keine Bewertungen
- OBII - 16 Postterm Pregnancy - PDF Version 1Dokument6 SeitenOBII - 16 Postterm Pregnancy - PDF Version 1Felina CabadingNoch keine Bewertungen
- Maternal Perception of Fetal Movements and Real-Time Ultrasound FindingsDokument6 SeitenMaternal Perception of Fetal Movements and Real-Time Ultrasound FindingsDarian AngNoch keine Bewertungen
- Understanding Molar Pregnancy and Gestational Trophoblastic DiseaseDokument55 SeitenUnderstanding Molar Pregnancy and Gestational Trophoblastic DiseaseClarains FriskaNoch keine Bewertungen
- Ob Post TestDokument11 SeitenOb Post TestAlexNoch keine Bewertungen
- Post Test 30 Items OBDokument5 SeitenPost Test 30 Items OBJohnasse Sebastian NavalNoch keine Bewertungen
- The Importance of Proteinuria in Preeclampsia and Its Predictive Role in Maternal and Neonatal OutcomesDokument9 SeitenThe Importance of Proteinuria in Preeclampsia and Its Predictive Role in Maternal and Neonatal OutcomesimuhammadfahmiNoch keine Bewertungen
- Placenta Increta Concept MapDokument1 SeitePlacenta Increta Concept MapEkay OrsolinoNoch keine Bewertungen
- Review of Maternal Mortality at A Tertiary Care Hospital - A One Year StudyDokument5 SeitenReview of Maternal Mortality at A Tertiary Care Hospital - A One Year StudyIJAR JOURNALNoch keine Bewertungen
- Assessment of The Factors Influencing Birth Preparedness and Complication Readiness Among Pregnant WomenDokument15 SeitenAssessment of The Factors Influencing Birth Preparedness and Complication Readiness Among Pregnant WomenTwinkleNoch keine Bewertungen
- HIGH RISK PREGNANCY FACTORS AND COMPLICATIONSDokument65 SeitenHIGH RISK PREGNANCY FACTORS AND COMPLICATIONSAthena Dela CruzNoch keine Bewertungen
- Stages of Labor BrochureDokument2 SeitenStages of Labor Brochureapi-273000494100% (1)
- Prenatal Workout Plan: GlowbodyptDokument10 SeitenPrenatal Workout Plan: GlowbodyptDébora BezerraNoch keine Bewertungen
- I So ImmunizationDokument21 SeitenI So ImmunizationaaaNoch keine Bewertungen
- Sample PRC RequirementsDokument4 SeitenSample PRC RequirementsRodney Beltran SubaranNoch keine Bewertungen
- Kesehatan Mental Masa PerinatalDokument37 SeitenKesehatan Mental Masa PerinatalluxNoch keine Bewertungen
- Obsteric EmergenciesDokument10 SeitenObsteric Emergenciestanmai nooluNoch keine Bewertungen
- Antenatal PalpationDokument2 SeitenAntenatal PalpationNandhiniNoch keine Bewertungen
- Management Placenta PreviaDokument24 SeitenManagement Placenta PreviaMuhammad RifaldiNoch keine Bewertungen
- Understanding the Bishop's Score for a Successful Labour InductionDokument2 SeitenUnderstanding the Bishop's Score for a Successful Labour InductionAndy WijayaNoch keine Bewertungen
- Sample First Trimester Twin Ultrasound ReportDokument2 SeitenSample First Trimester Twin Ultrasound ReportPriyankaNoch keine Bewertungen
- Coding ICD Yossi PDFDokument3 SeitenCoding ICD Yossi PDFYossi Agung AriosenoNoch keine Bewertungen
- Womens Health Field EncountersDokument17 SeitenWomens Health Field EncountersFelix OmondiNoch keine Bewertungen
- Early Pregnancy Physical RisksDokument4 SeitenEarly Pregnancy Physical RisksDham DoñosNoch keine Bewertungen
- PartoghraphDokument60 SeitenPartoghraphharley dela cruzNoch keine Bewertungen
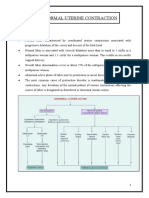
- Abnormal Uterine Actions - Monika MakwanaDokument10 SeitenAbnormal Uterine Actions - Monika Makwanamonika makwanaNoch keine Bewertungen
- Jurnal PEDokument7 SeitenJurnal PEIris BerlianNoch keine Bewertungen
- Nama: Nadia Fitra RahmaDokument2 SeitenNama: Nadia Fitra RahmaNadya Fitra RahmaNoch keine Bewertungen
- Healing PCOS: A 21-Day Plan for Reclaiming Your Health and Life with Polycystic Ovary SyndromeVon EverandHealing PCOS: A 21-Day Plan for Reclaiming Your Health and Life with Polycystic Ovary SyndromeNoch keine Bewertungen
- What to Expect When You’re Expecting (5th Edition)Von EverandWhat to Expect When You’re Expecting (5th Edition)Bewertung: 5 von 5 Sternen5/5 (1)
- The Longevity Book: The Science of Aging, the Biology of Strength, and the Privilege of TimeVon EverandThe Longevity Book: The Science of Aging, the Biology of Strength, and the Privilege of TimeBewertung: 3.5 von 5 Sternen3.5/5 (13)
- What No One Tells You: A Guide to Your Emotions from Pregnancy to MotherhoodVon EverandWhat No One Tells You: A Guide to Your Emotions from Pregnancy to MotherhoodBewertung: 4.5 von 5 Sternen4.5/5 (30)
- The Menopause Manifesto: Own Your Health With Facts and FeminismVon EverandThe Menopause Manifesto: Own Your Health With Facts and FeminismBewertung: 4 von 5 Sternen4/5 (18)
- Period Power: Harness Your Hormones and Get Your Cycle Working For YouVon EverandPeriod Power: Harness Your Hormones and Get Your Cycle Working For YouBewertung: 4 von 5 Sternen4/5 (25)
- All in Her Head: The Truth and Lies Early Medicine Taught Us About Women’s Bodies and Why It Matters TodayVon EverandAll in Her Head: The Truth and Lies Early Medicine Taught Us About Women’s Bodies and Why It Matters TodayBewertung: 5 von 5 Sternen5/5 (2)
- The Pain Gap: How Sexism and Racism in Healthcare Kill WomenVon EverandThe Pain Gap: How Sexism and Racism in Healthcare Kill WomenBewertung: 4 von 5 Sternen4/5 (153)
- ADHD Women: A Holistic Approach To ADHD ManagementVon EverandADHD Women: A Holistic Approach To ADHD ManagementBewertung: 5 von 5 Sternen5/5 (4)
- Summary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisVon EverandSummary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisBewertung: 3 von 5 Sternen3/5 (2)
- Kitchen Witch: Food, Folklore & Fairy TaleVon EverandKitchen Witch: Food, Folklore & Fairy TaleBewertung: 4 von 5 Sternen4/5 (2)
- Brain Body Diet: 40 Days to a Lean, Calm, Energized, and Happy SelfVon EverandBrain Body Diet: 40 Days to a Lean, Calm, Energized, and Happy SelfBewertung: 5 von 5 Sternen5/5 (2)
- The Autoimmune Cure: Healing the Trauma and Other Triggers That Have Turned Your Body Against YouVon EverandThe Autoimmune Cure: Healing the Trauma and Other Triggers That Have Turned Your Body Against YouNoch keine Bewertungen
- Younger Next Year, 2nd Edition: Live Strong, Fit, Sexy, and Smart-Until You're 80 and BeyondVon EverandYounger Next Year, 2nd Edition: Live Strong, Fit, Sexy, and Smart-Until You're 80 and BeyondBewertung: 4 von 5 Sternen4/5 (110)
- Breaking Free from Body Shame: Dare to Reclaim What God Has Named GoodVon EverandBreaking Free from Body Shame: Dare to Reclaim What God Has Named GoodBewertung: 5 von 5 Sternen5/5 (33)
- I'm So Effing Tired: A Proven Plan to Beat Burnout, Boost Your Energy, and Reclaim Your LifeVon EverandI'm So Effing Tired: A Proven Plan to Beat Burnout, Boost Your Energy, and Reclaim Your LifeBewertung: 4 von 5 Sternen4/5 (15)
- The Path of the Priestess: A Guidebook for Awakening the Divine FeminineVon EverandThe Path of the Priestess: A Guidebook for Awakening the Divine FeminineBewertung: 4 von 5 Sternen4/5 (2)
- Not a Diet Book: Take Control. Gain Confidence. Change Your Life.Von EverandNot a Diet Book: Take Control. Gain Confidence. Change Your Life.Bewertung: 4.5 von 5 Sternen4.5/5 (124)
- The Hormone Secret: Discover Effortless Weight Loss and Renewed Energy in Just 30 DaysVon EverandThe Hormone Secret: Discover Effortless Weight Loss and Renewed Energy in Just 30 DaysBewertung: 4.5 von 5 Sternen4.5/5 (5)
- The First Forty Days: The Essential Art of Nourishing the New MotherVon EverandThe First Forty Days: The Essential Art of Nourishing the New MotherBewertung: 5 von 5 Sternen5/5 (5)
- A Radical Guide for Women with ADHD: Embrace Neurodiversity, Live Boldly, and Break Through BarriersVon EverandA Radical Guide for Women with ADHD: Embrace Neurodiversity, Live Boldly, and Break Through BarriersBewertung: 4.5 von 5 Sternen4.5/5 (71)
- Bumpin': The Modern Guide to Pregnancy: Navigating the Wild, Weird, and Wonderful Journey From Conception Through Birth and BeyondVon EverandBumpin': The Modern Guide to Pregnancy: Navigating the Wild, Weird, and Wonderful Journey From Conception Through Birth and BeyondBewertung: 4.5 von 5 Sternen4.5/5 (38)
- Women, Food, And Hormones: A 4-Week Plan to Achieve Hormonal Balance, Lose Weight, and Feel Like Yourself AgainVon EverandWomen, Food, And Hormones: A 4-Week Plan to Achieve Hormonal Balance, Lose Weight, and Feel Like Yourself AgainBewertung: 4 von 5 Sternen4/5 (14)
- The Mama Natural Week-by-Week Guide to Pregnancy and ChildbirthVon EverandThe Mama Natural Week-by-Week Guide to Pregnancy and ChildbirthBewertung: 4.5 von 5 Sternen4.5/5 (21)
- Stopping Stress Before It Stops You: A Game Plan for Every MomVon EverandStopping Stress Before It Stops You: A Game Plan for Every MomBewertung: 4.5 von 5 Sternen4.5/5 (20)
- 9 Months Is Not Enough: The Ultimate Pre-Pregnancy Checklist to Create a Baby-Ready Body and Build Generational HealthVon Everand9 Months Is Not Enough: The Ultimate Pre-Pregnancy Checklist to Create a Baby-Ready Body and Build Generational HealthNoch keine Bewertungen
- The Better Period Food Solution: Eat Your Way to a Lifetime of Healthier CyclesVon EverandThe Better Period Food Solution: Eat Your Way to a Lifetime of Healthier CyclesNoch keine Bewertungen